Article Text

Statistics from Altmetric.com
Description
A woman aged 66 years with a history of diplopia, headaches and left Cranial Nerve 3 palsy was found to have a 2 cm left paraclinoid internal carotid artery aneurysm. She was started on aspirin and clopidogrel and underwent flow diversion treatment with Pipeline (Covidien Neurovascular, Irvine, California, USA) embolisation of the aneurysm. Intraoperative neurophysiological monitoring via EEG and somatosensory evoked potentials was performed. After the procedure, she was found to have a large right scalp haematoma extending to the right orbit anteriorly and the back of the head posteriorly. Despite manual compression, the periorbital swelling continued to increase in the intensive care unit such that she was not able to open the right eye. A routine postprocedural MRI and MRA of the brain with gadolinium was performed to assess the aneurysm; of note, the study also demonstrated a large right scalp haematoma with contrast enhancement around the superficial temporal artery (STA) consistent with extravasation (figures 1 and 2). A delayed sequence was not performed to distinguish between the pseudoaneurysm and active haemorrhage, but given the enlargement of the haematoma before and after the MRI, active haemorrhage is favoured. The site of enhancement was where one of the electrodes had been placed for intraoperative monitoring, suggesting that the electrode had punctured the STA. The patient's head was wrapped with woven gauze soaked in epinephrine and saline. By postoperative day 2, the swelling had significantly decreased, and she was able to open her right eye.

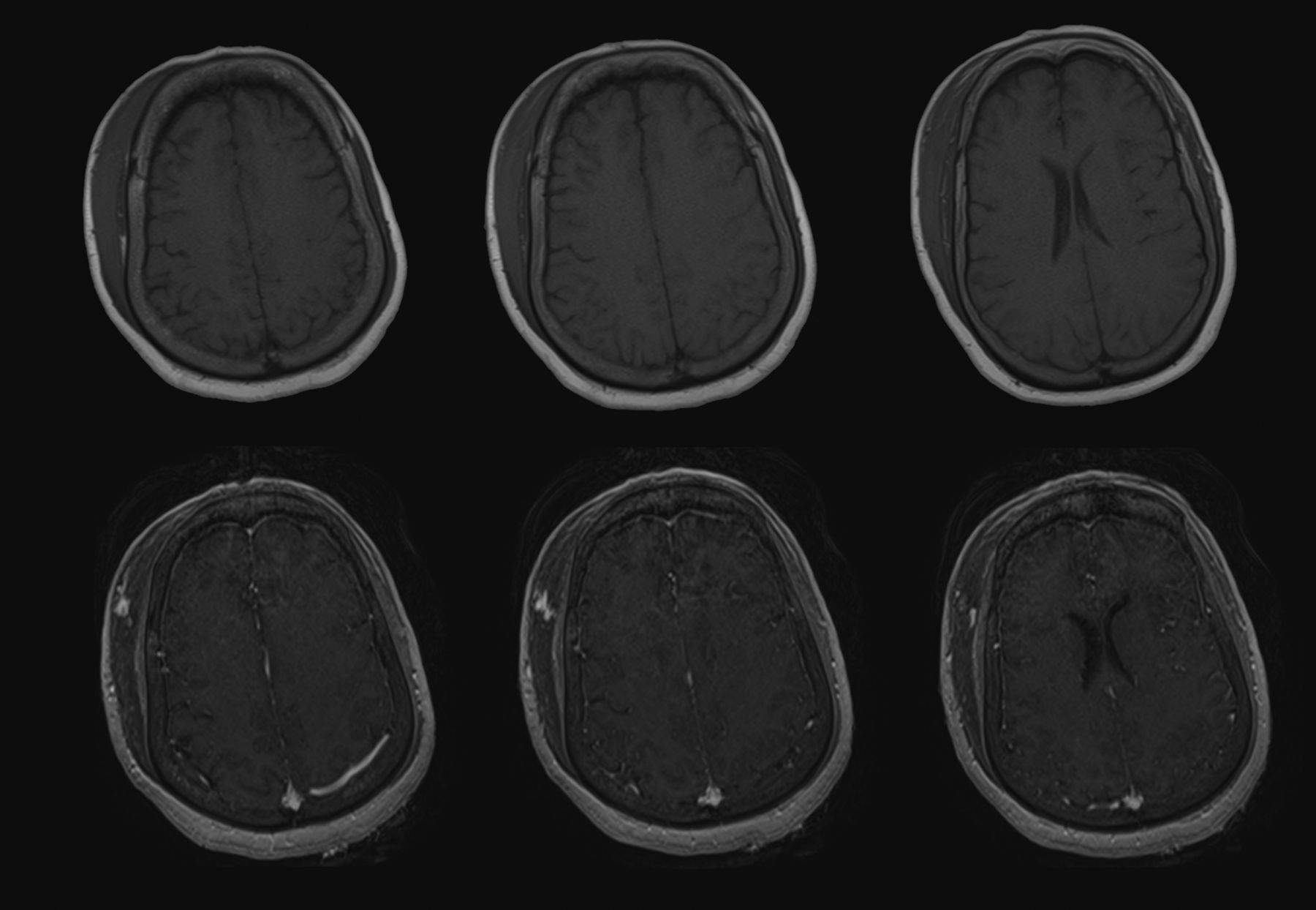
Axial, T1-weighted, precontrast (top row) and postcontrast (bottom row) images progressing from superior (left) to inferior (right) demonstrate contrast enhancement within a right scalp haematoma.

{kind=link}
{kind=link}
Sagittal, postcontrast, T1-weighted images progressing from lateral (left) to medial (right) show contrast enhancement arising at the right superficial temporal artery and extending posteriorly and inferiorly within the right scalp hematoma.
Intraoperative neurophysiological monitoring has been shown to be useful for endovascular embolisation procedures,1 but data on adverse events caused by neurophysiological monitoring are limited. Haemorrhagic complications in patients taking antiplatelet agents following Pipeline embolisation procedures have been documented,2 but STA haemorrhage from scalp electrode insertion has not been reported.
Learning points
Arterial injury is a potential complication of neurophysiological monitoring which can have especially deleterious consequence in patients taking antiplatelet agents.
Compression and local, transdermal epinephrine is a treatment strategy for controlling superficial temporal artery haemorrhage in patients who continue with antiplatelet agents to prevent stent thrombosis.
Footnotes
Contributors GWP performed the literature review, drafted the manuscript and selected images. RG saw the patient in clinic, performed the patient's procedure and edited the manuscript and figures. WCP and SH treated the patient's haematoma in the intensive care unit and contributed to and edited the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.