Article Text

Statistics from Altmetric.com
Description
A sinus of Valsalva aneurysm (SVA) is an uncommon cardiac anomaly that can be congenital or acquired. SVAs were present in 0.09% of cadavers in a large autopsy series and ranged between 0.14–0.23% in a Western surgical series.1 A congenital SVA is usually clinically silent but may vary from a mild, asymptomatic dilation detected in routine two-dimensional echocardiography, to symptomatic presentations related to the compression of adjacent structures or intracardiac shunting caused by rupture of the SVA into the right side of the heart. Approximately 65–85% of SVAs originate from the right sinus of Valsalva, while SVAs originating from non-coronary (10–30%) and left sinuses (<5%) are exceedingly rare.
The most common complication is rupture into the atrium or ventricle, and, very rarely, towards the left chambers, causing left-to-right shunting or aortic valve insufficiency with congestive heart failure and the need for urgent surgical resolution. Although open-heart surgery with or without aortic valve replacement remains the treatment of choice, trans-catheter device closure of a ruptured SVA has been successfully performed.2 So far, around 136 cases of device closure of ruptured SVAs have been reported in the literature.3 For an asymptomatic unruptured SVA, there is no consensus regarding management. Most large surgical series have advocated early surgical repair even if the patient is asymptomatic, while Vural et al3 proposed that patients with unruptured, stable aneurysms should be anticoagulated, followed at 6-month intervals, and then repaired if symptoms develop or the size of the sinus is >50% of the average size of the other two normal Valsalva sinuses, compresses or distorts surrounding chambers or tissues, or increases in consecutive echocardiographic examinations.
We present a case of a 34-year-old man with acute heart failure symptoms of 1 week duration. Transthoracic echocardiogram revealed a ruptured sinus of Valsalva aneurysm entering into the right ventricle (figure 1). Angiogram revealed a classical windsock deformity (figure 2 and video 1). Successful device closure was achieved using a 10/12 mm LIFETECH CERA PDA occlusion device. Subsequent angiogram and echocardiogram revealed no residual shunt (figures 3 and 4, and video 2). The patient was on regular follow-up for 6 months and did not have any recurrence of symptoms.

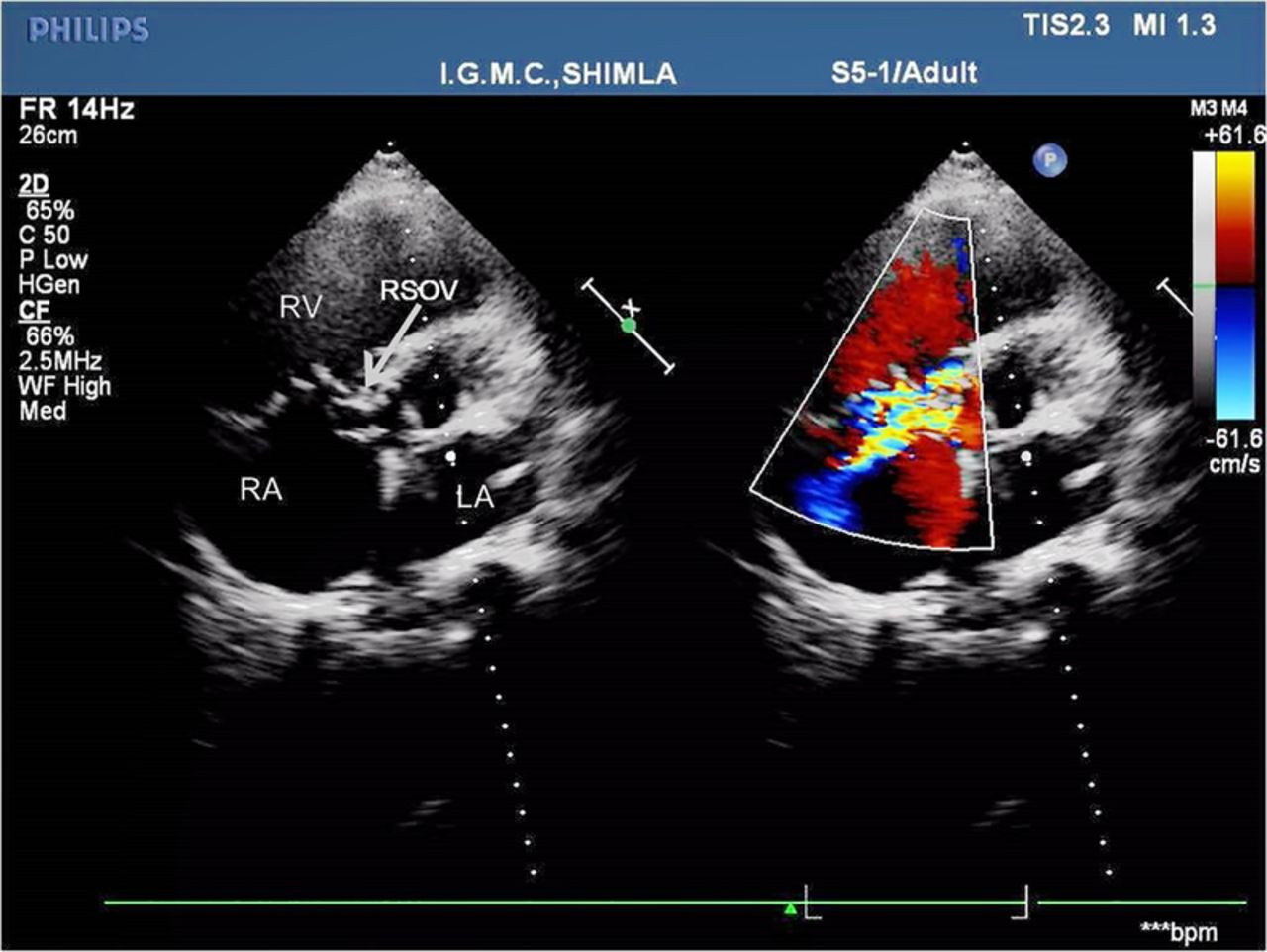
Transthoracic echocardiogram, parasternal short-axis view, displaying an RSOV (arrow), with colour Doppler demonstrating shunting into the right atrium (RA) near the tricuspid valve (LA, left atrium; RSOV, ruptured sinus of Valsalva; RA, right atrium; RV, right ventricle).

Aortic root angiogram showing a ruptured sinus of Valsalva aneurysm forming a windsock deformity (arrow) into the right side chambers.

Aortic root angiogram showing the device (arrow) positioned across the ruptured sinus of Valsalva just before its deployment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transthoracic echocardiogram, apical four- chamber view, showing the device in situ (arrow) across the RSOV (LA, left atrium; LV, left ventricle; RSOV, ruptured sinus of Valsalva; RA, right atrium; RV, right ventricle).
Aortic root angiogram showing opacification of the right ventricle on aortic root injection through the ruptured sinus of Valsalva.
Aortic root angiogram showing no residual shunt across the ruptured sinus of Valsalva after device deployment.
Learning points
Ruptured sinus of Valsalva aneurysm is a rare cardiac anomaly.
Presentation varies from asymptomatic findings to acute heart failure, which can rapidly worsen to cause death.
Although surgery is the gold standard treatment, percutaneous transcatheter closure has now become equally efficacious with fewer complications.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.