Article Text

Statistics from Altmetric.com
Description
A 70-year-old man presented to a community hospital in the northern Mid-Atlantic US midsummer with a main problem of severe, stabbing, knife-like pain behind the left eye and a little bit behind the right eye which had started a few days ago but abruptly worsened at 3 o’clock in the morning. He also had a change in the colour perception in his left eye and double vision, which improved when a patch was placed on his left eye. On physical examination, there was moderate left lateral gaze palsy. Funduscopy was not performed. The remainder of the neurologic and ocular examinations was normal. On physical examination, a 15 cm, erythematous, left subaxillary patch resembling a bullseye was incidentally visualised (figure 1).

The patient exhibits a 15 cm erythematous, blanchable, non-pruritic, non-painful, subaxillary bulls-eye patch which he had not noticed and was only visualised on presentation. This photograph was taken 2 days later, by which time the rash’s size and redness had diminished considerably.
Medical history was remarkable for stage IV adenocarcinoma of unknown primary diagnosed 6 years prior, assumed to be gastrointestinal per standard practice since below the diaphragm (or possibly pancreaticobiliary), for which the patient was started treatment for with FOLFOX and then FOLFIRI. The most recent chemotherapy was 11 days ago with FOLFIRI and a single dose of dexamethasone. He also had a history of deep venous thrombosis of the left leg a few years ago and superior mesenteric vein thrombosis 6 months ago (currently on anticoagulation), diabetes mellitus, and cirrhosis. There was no history of optic neuritis, multiple sclerosis, nerve problems or autoimmune disease. Despite the patient’s comorbidities, he was active and of excellent performance status.
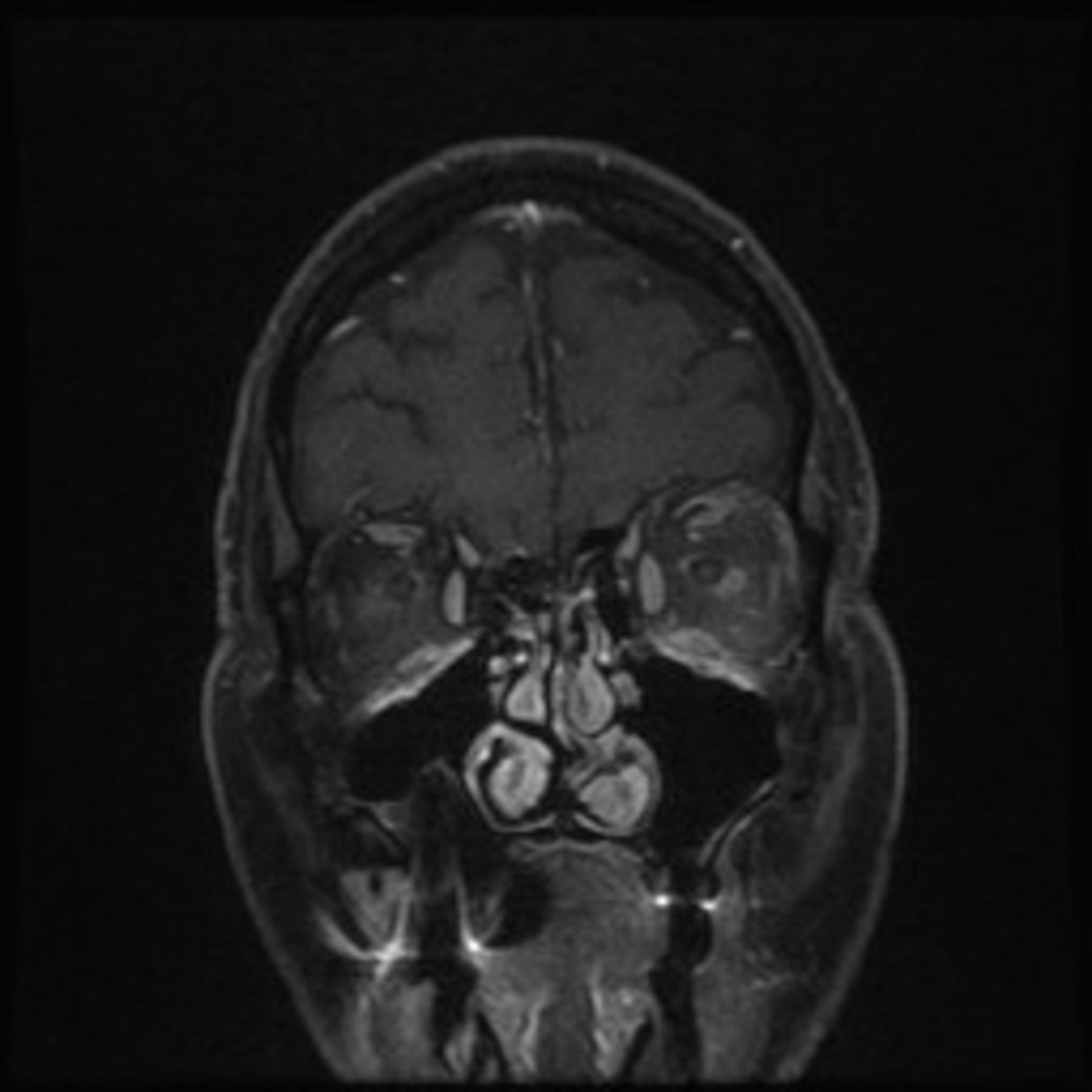
Lyme disease serum serology using LIAISON quantitative chemiluminescence was positive at 3.45 index for IgG and IgM to Borrelia burgdorferi (reference is <1). Second-stage testing with western blot was omitted because further specificity was not needed, given the patient’s stereotypical erythema migrans (EM) and the rather high incidence of false negatives in the western blot (occurring as often as 50% of the time in some circumstances).1–3 EM in high-risk patients, such as ours, is specific for Lyme disease and antimicrobial therapy is indicated independent of any tests (which are often not even performed outpatient, as they are frequently falsely negative in the acute window period).1 3 4 The patient, who lived in a wooded area with deer, did not recall any tick exposure; however, only one out of every four patients with Lyme disease do.5 In any case, cerebrospinal fluid (CSF) was clear and colourless with a total cell count of 20: 1 neutrophil, 15 lymphocytes and 4 monocytes. There were zero erythrocytes. CSF total protein and glucose were both 67 mg/dL. CSF Lyme disease antibody, using the same chemiluminescence study as for the serum, was borderline at 0.127 (reference <0.117). MRI of the brain and orbits with and without contrast (figures 2 and 3) showed enhancement of the left optic sheath most pronounced along the orbital segment of the left optic nerve, just proximal to the intraorbital segment. Since the patient had the typical EM rash and it responded to treatment, more extensive workup for optic neuritis was not pursued. Abducens nerve palsy also frequently occurs in diabetes mellitus, but this was considered less likely with the EM rash. Intravenous ceftriaxone was initiated for Lyme disease as well as empiric doxycycline for any possible concurrent subclinical rickettsial zoonosis. Corticosteroids were not used because the optic perineuritis was thought to be secondary to the Lyme disease. The patient’s EM abated and his neuro-ophthalmologic symptoms improved. He was discharged 3 days later to complete a course of 4 weeks of intravenous ceftriaxone and his symptoms did not recur.

MRI shows prominent asymmetric enhancement of the left optic sheath most pronounced along the orbital segment of the left optic nerve, just proximal to the intraorbital segment. A coronal view.

{kind=link}
{kind=link}
{kind=link}
MRI shows prominent asymmetric enhancement of the left optic sheath most pronounced along the orbital segment of the left optic nerve, just proximal to the intraorbital segment. An axial view.
This case is important because while abducens nerve palsy or multifocal disease is not atypical of neuroborreliosis,6 optic neuritis in association with Lyme disease is rare.7 In 2005, retrospective data suggested that optic neuritis occurs rarely secondary to Lyme disease.8 Authors of a 2007 report of active Lyme disease associated with optic neuritis cautiously prefaced their case by informing the reader that none of 14 previous cases in the literature that they examined fulfilled the Halperin or Sibony criteria for active Lyme disease.9 However, since that time, more cases have emerged describing optic neuritis due to underlying Lyme disease.10 11 This case is interesting because the perineuritis symptoms resemble optic neuritis.
As a side note, this case is also interesting because the EM presented at the same time as the neuro-ophthalmologic symptoms. Human spirochetal illnesses (such as those caused by Treponema, Leptospira or Borrelia) are classically characterised as having three distinct clinical stages.12 13 EM is a sign of early, localised disease, most often appearing within a month after infection, whereas arthritis, carditis and neurological disease are typical of later stages. The positive serology in our patient suggests that the patient had been infected by B. burgdorferi already for some time before the EM appeared. Perhaps some of the presentation can be explained by the patient’s immunosuppression. Another interesting feature of this case is that the patient had some mild symptoms in his second eye, and bilaterality is a feature sometimes observed in Lyme disease (such as in Lyme cranial neuropathy)13 14 as opposed to in other neurologic disorders.
We were fortunate that our patient had EM, which made our diagnosis and treatment relatively straightforward. However, only 80% of patients with Lyme disease develop EM2 15 and it usually occurs in the early, localised stage. As such, some readers may interpret this case as supporting keeping Lyme disease on the differential.
Learning points
While it may have been a concurrence, this case may demonstrate a rare manifestation of Lyme neuroborreliosis: optic perineuritis (together with abducens palsy and erythema migrans (EM)).
Eighty per cent of the time, Lyme disease initially presents with a bulls-eye rash named EM, which is a quite specific feature. However, Lyme disease sometimes does not present with EM and can linger to present later with various manifestations, including neurologic, rheumatologic and cardiac disease.
Acknowledgments
We wish to acknowledge Charles Elkin MD in the department of radiology at our institution.
References
Footnotes
Contributors ML wrote the manuscript. SS edited and revised the manuscript twice, making substantial changes. CS and DS saw the patient, reviewed the manuscript and gave substantial input.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.