Article Text

Statistics from Altmetric.com
Description
This 79-year-old woman was involved in a road traffic collision in which another driver rear-ended her stationary car at a speed of around 70 m/h. She was transferred to the nearest Major Trauma Centre, where her observations remained stable and initial primary survey was unremarkable. She had a full trauma CT that revealed extensive bilateral rib fractures with flail of 8+9 on the left, a C4-5 body fracture and, most significantly an acute traumatic pseudoaneurysm of the thoracic aorta and associated pneumomediastinum.
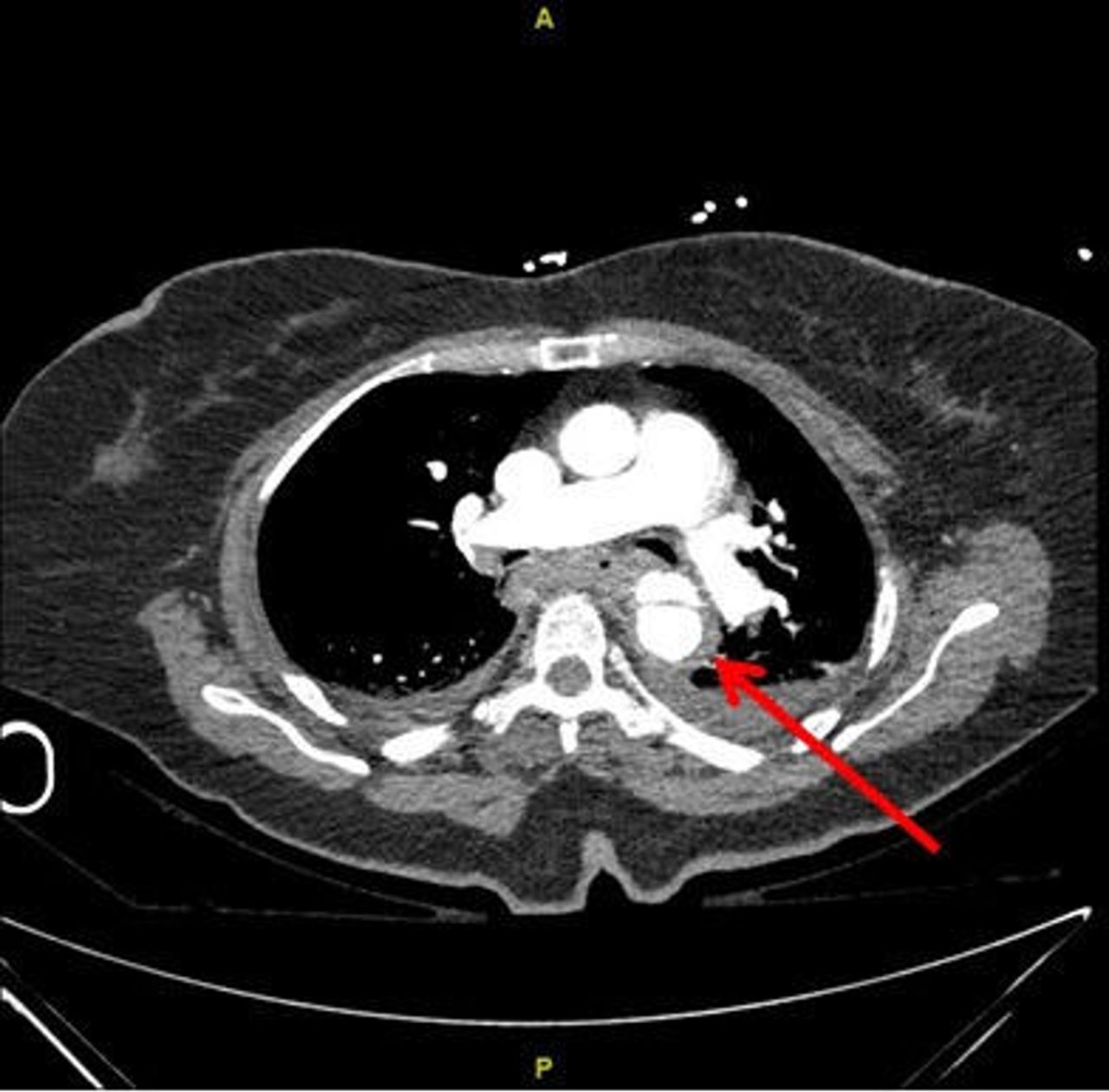
The CT images show transverse and coronal views of this pseudoaneurysm. On the coronal views(figure 1), you can see a bulging of the anterior wall of the thoracic aorta, just below the level of the isthmus. On the transverse view(figure 2), you can see the lumen of the aorta (indicated by an arrow), with a false lumen demonstrating dissection of this vessel.

This sagittal view shows an outpouching of the thoracic aorta along the underside of the aortic isthmus, in keeping with an anterior traumatic pseudoaneurysm.

{kind=link}
{kind=link}
Axial view. The pseudoaneurysm sac measures 2.5×1 cm and is indicated by the arrow. Surrounding periaortic haematoma and hyperdense fluid within the mediastinum and pleural spaces, in keeping with haemomediastinum and haemothorax.
A discussion was held with interventional radiology, who recommended endovascular stenting of the injured aorta under general anaesthetic to minimise the chances of future rupture. The anaesthetic team however deemed her very high risk given her trauma burden coupled with her advanced age and significant pre-existing comorbidities. They advised us that she was unlikely to survive a general anaesthetic. This was discussed fully with the patient who did not want to risk a general anaesthetic, due to the low probability of survival, before she has had the chance to see her family. She was therefore admitted to the ward with an Aspen collar for her C4-5 fracture and epidural for pain relief from her ribs. Over the next day, she began to deteriorate with her breathing, and unfortunately passed away rapidly the following night, with high suspicion of rupture of her pseudoaneurysm.
In blunt trauma, this injury more commonly occurs from a deceleration injury and located around the aortic isthmus as this is the point where the thoracic aorta, which is relatively mobile, joins with the arch of aorta which is fixed.1 2 The majority of patients with traumatic injury to the thoracic aorta tend to die on scene or before arrival to hospital.3 In this case, the patient arrived in an apparently stable condition, not showing any signs of obvious injury. It was only on CT scanning, which was done due to high impact trauma combined with old age and frailty that her injuries were picked up. On another occasion, this could very easily have been missed.
Learning points
Beware of ‘normal’ observations in geriatric trauma—older people can present as haemodynamically stable following trauma despite significant injury due to polypharmacy, medical conditions such as hypertension or limited physiological reserve.
Importance of multidisciplinary team (MDT) involvement in trauma—Major Trauma team, radiology, vascular and anaesthetics involved in making decision that she would be unsuitable for general anaesthesia and endovascular intervention due to poor physiological reserve with high trauma burden
Ensure to involve the patient in decisions where possible. In this case, decision had been made by the MDT, but patient was in agreement with decision.
Ethics statements
Acknowledgments
We would like to thank to Mr Brooks and Dr Freij for their support and encouragement in writing this report.
Footnotes
Twitter @AngeloLaValle6
Contributors MH and ALV reviewed the literature on the subject, wrote the case report and selected the appropriate images. RF and AB reviewed the drafts and supervised the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.