Article Text

Statistics from Altmetric.com
Description
We have devised a novel technique for intraoperative fundus assessment which we routinely use in our paediatric cataract surgery cases. After the routine steps of paediatric lens aspiration, just before the intraocular lens (IOL) is implanted (or other ways if aphakia is planned for), we insert a 25-gauge endoilluminator routinely used for vitreoretinal surgeries (commonly involving LED (light-emitting diode) bulbs)1 through one of the self-sealing corneal side ports in the bag after filling it with viscoelastic if posterior rhexis is not done and into the anterior vitreous cavity after limited anterior vitrectomy in case posterior capsulorhexis has been done (figure 1). A contact lens for wide-angle viewing is placed on the cornea coupled with viscoelastic.1 We commonly use MiniQuad lens (Volk Optical), which has a magnification of 0.48× with a static field of 106° and a dynamic field of 127°.1 We have recorded numerous posterior segment findings. Figure 2 shows the posterior segment anomalies detected intraoperatively in four children with total white cataract. All the manoeuvres are done using sterile surgical instruments, minimising the risk of any infection. The endoilluminator and the wide-angle viewing lens are sterile and are the same as that normally used during vitrectomy. To date, we have not had any sort of infective inflammation in any of the paediatric cataract surgery eyes in which this posterior segment evaluation technique was used. IOL is implanted and/or the wound is closed/sutured normally after viscoaspiration.

The steps of our technique. (A) Lens aspiration is done with bimanual irrigation and aspiration probes. (B) Posterior curvilinear capsulorhexis is done with 25-gauge intravitreal forceps. (C) Limited anterior vitrectomy is done. (D) Bag filled with viscoelastic. (E,F) 25-gauge illuminator being injected through the side port.
{kind=link}
{kind=link}
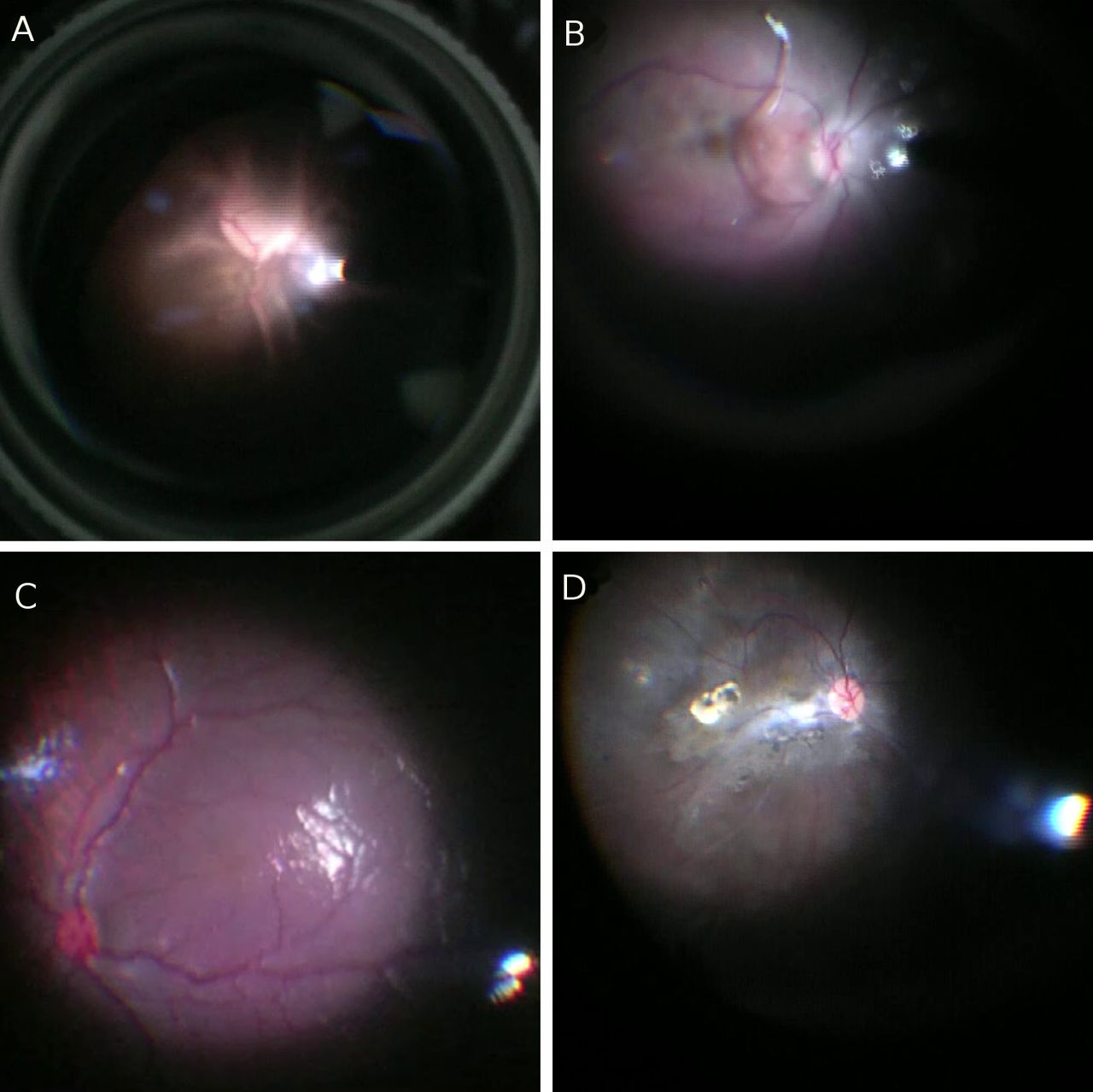
(A) Closed funnel retinal detachment in a 24-month-old child. (B) Vascular stalk of persistent fetal vasculature in an 8-month-old child. (C) Foveal hypoplasia in a case of aniridia in a 30-month-old child. (D) Toxoplasmosis macular scar in a 15-month-old child.
Our technique has the advantage of allowing for documentation and teaching and providing a fundus view through a clear media (corneal and vitreous opacities excluded) which cannot be in any way compared with what is visible even through a mildly cataractous lens. It can also prognosticate cases and we know what visual potential to expect postoperatively. Documentation of posterior segment findings usually requires expensive machinery, such as traditional fundus cameras, RetCam and Optos. Our technique is simple and allows recording even in the most basic ophthalmic surgical theatres with an operating microscope, wide-angle lens and a light source. Patient cooperation is not a hindrance and neither are associated involuntary ocular movements like nystagmus. A decent view of the fundus is possible even in poorly dilating pupils because the source of illumination is in the posterior segment itself. Intraoperative video recordings are routinely practised by posterior segment surgeons, and we have used the same basic principles and modified them a bit to be used as a novel and ergonomic method by anterior segment surgeons during cataract surgeries.
Learning points
Fundus evaluation is a must to prognosticate cataract surgery cases postoperatively.
The posterior segment visualisation technique using wide-angle viewing system during vitrectomy can also be modified and used during anterior segment surgeries.
Ethics statements
Patient consent for publication
Footnotes
Contributors SK: concept, surgery. AAB: preparation of the manuscript. TS: video editing. MB: editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.