Article Text

Statistics from Altmetric.com
Description
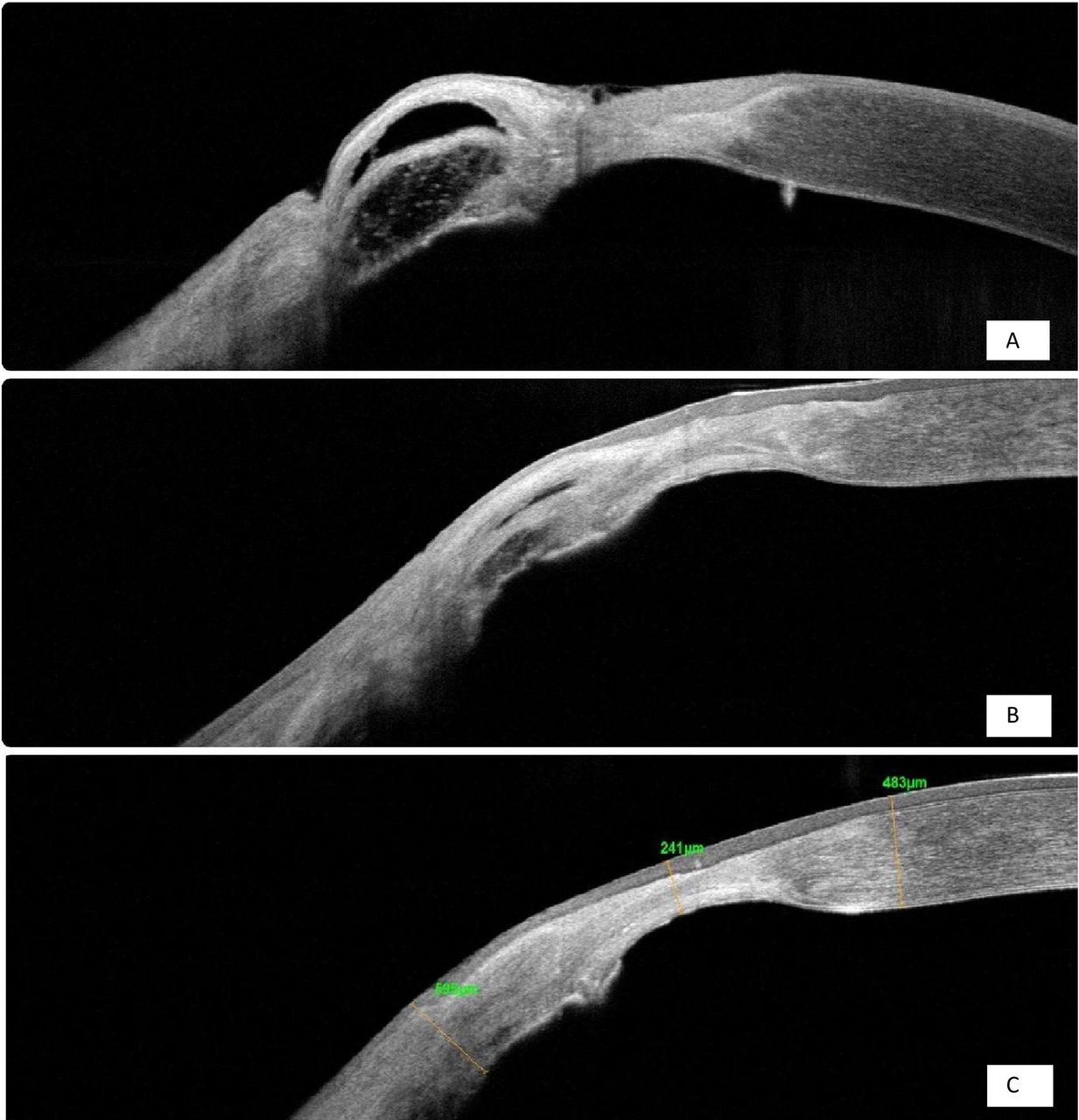
A 19-year old man with a peripheral corneal scar in left eye (LE) status post microbial keratitis 1 year ago developed perforation at the site of the scar after a recent injury with a finger. Cyanoacrylate tissue adhesive (TA) application with bandage contact lens (BCL) placement was done locally prior to referral to us. On examination, visual acuity in LE was 20/100 (20/50 with pinhole). TA was dislodged from its place and circular perforation of size 1–2 mm close to the limbus at 8 o’clock, with surrounding vascularised scar and irregular anterior chamber (AC) depth were noted (figure 1A). The right eye (RE) was within normal limits. TA BCL application with AC reformation was done in LE. Six weeks later, he had to undergo repeat procedure for a similar situation. Subsequently, AC remained well formed for the next 3 months when it was decided to remove TA in the operating room. After removal of TA, unhealed perforation with punched-out edges was noted underneath. The epithelium surrounding the perforation was removed. An amniotic membrane folded on itself three times was used to cover the perforation and was secured to the cornea with 10–0 nylon overlay sutures (multilayered amniotic membrane graft (mAMG)) (figure 1B,C). Fibrin glue was used in between layers of amniotic membrane. AC was formed with saline and small air bubble and a BCL was placed. On postoperative day 1, he required replacement of one loose suture. He received a prophylactic antibiotic and lubricating eye drops postoperatively. Subsequently over next 6 months, sutures were removed and the amniotic membrane became integrated within the stroma. He underwent left eye lens aspiration with posterior chamber intraocular lenses (PC IOL) implantation for complicated cataract 10 months after mAMG (figure 1D). Best-corrected visual acuity 6 months after cataract surgery was 20/20 p. Serial anterior segment optical coherence tomography (AS-OCT) scans over a 7-month period shows a relatively hyper-reflective signal in the healed region of a previous fistula, indicating integration of multilayered amniotic membrane into corneal stroma (figure 2A–C)
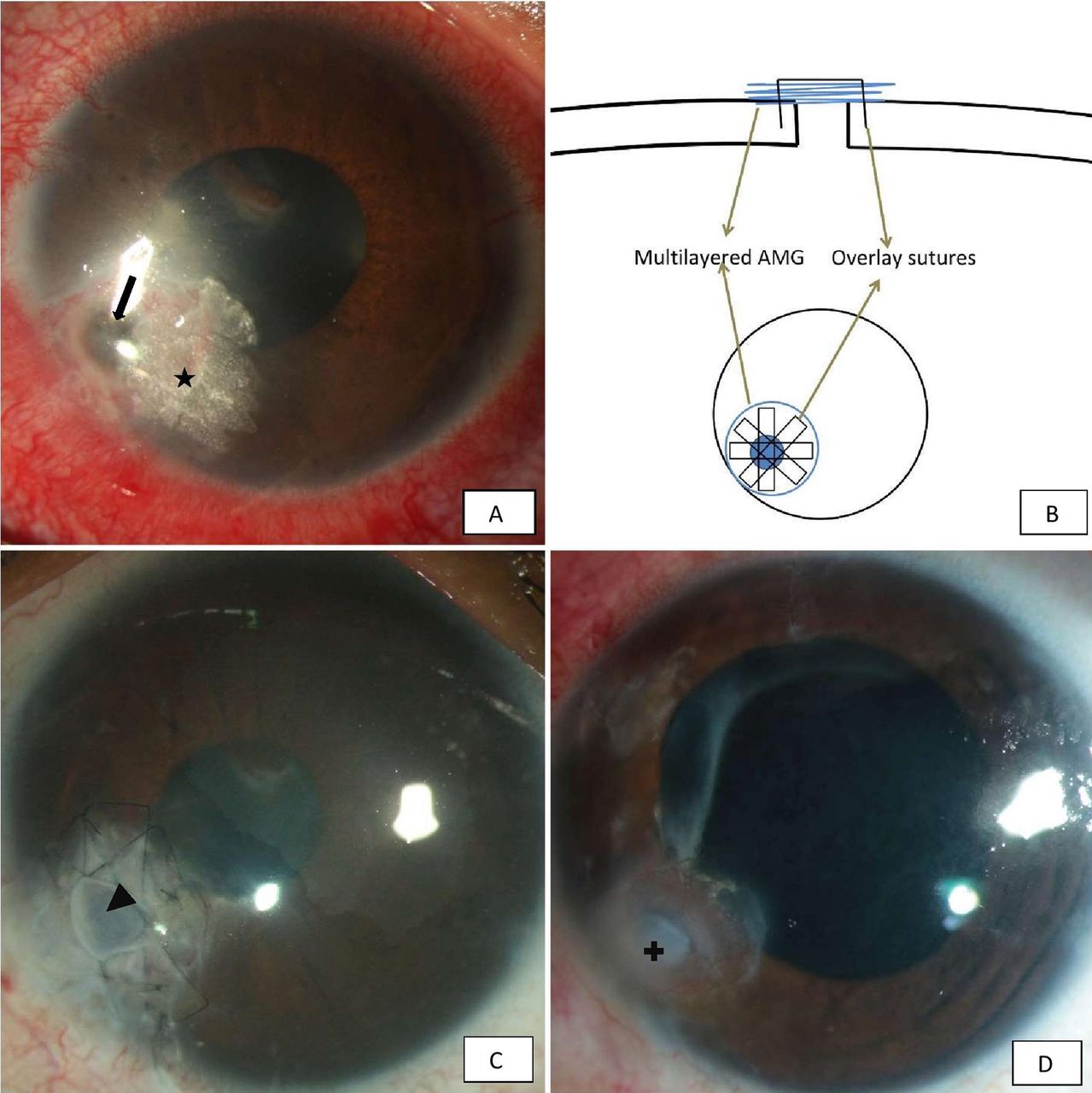
(A) Corneal perforation (arrow) with dislodged TA (star) and adjacent vascular scar. (B) Technique of mAMG with overlay sutures (illustrative diagram). (C) 1 week postoperation: mAMG with overlay sutures showing ballooning over area of peroration (arrowhead). (D) After 1 year: healed perforation with integrated amniotic membrane (plus). mAMG, multilayered amniotic membrane graft; TA, tissue adhesive.

{kind=link}
{kind=link}
Serial anterior segment optical coherence tomography scans showing progressive integration of multilayered amniotic membrane graft into the corneal stroma closing the chronic fistula. Postoperative duration (A) 6 weeks, (B) 4 months and (C) 7 months.
A corneal fistula is a communication between the AC and the corneal surface.1 Corneal fistula follows either trauma or perforation in corneal ulcer, infected or sterile. The defect does not heal spontaneously because of the combined poor tissue apposition and persistent aqueous humour flow.1 Persistence of perforation can lead to potentially devastating complications like peripheral anterior synechiae formation, secondary glaucoma, prolonged or recurrent hypotony, phthisis bulbi, endophthalmitis or panophthalmitis. The management of a corneal perforation includes tissue glues, mAMGs, Tenon’s patch and tectonic corneal grafts, depending on the size, shape, location, cause of the lesion, the surgeon’s experience and the availability of tissue.2 3 Amniotic membrane transplantation, if used for corneal perforation, can prevent urgent penetrating keratoplasty. Its application can restore stromal thickness and its advantage is that it can be stored in appropriate conditions for many months. Various authors have reported good final functional result following use of the multilayered amniotic membrane transplantation.4 5 The limitation of using AMG is that it is an opaque tissue. Thus, in patients with perforation involving the centre of the cornea, visual acuity may not improve in spite of adequate healing.
Learning points
Multilayer amniotic membrane transplantation is an effective method for the treatment corneal perforations.
The biological properties of amniotic membrane make it a useful tool for the reconstruction of damaged corneal tissue to restore its integrity.
Acknowledgments
I thank my institute, L V Prasad Eye Institute, which has given me the foundation for making this report.
Footnotes
Contributors RPP and PK were involved in creating the content and organising the images of this report. RPP conceptualised the paper. PK managed the patient and also acquired the images. PK is the overall guarantor of the paper.
Funding Hyderabad Eye Research Foundation, India.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.