Article Text

Statistics from Altmetric.com
Description
A 27-year-old woman, known case of Takayasu Arteritis on systemic immunosuppression, was referred by her rheumatologist for ocular evaluation as the patient had problems of floaters and diminution of vision in both eyes since 1 month. She had bilateral occlusion (>80%) of her carotid arteries and had been started on low molecular weight heparin by her treating physician. On examination, her best corrected visual acuity (BCVA) was 20/100 N6 in the right eye and 20/125, N6 in left eye. The anterior segment examination of both eyes was essentially normal. Intraocular pressure in right and left eyes was 12 mm Hg and 13 mm Hg, respectively. Pupils in both eyes were sluggishly reacting to light. Fundus examination of both eyes (figure 1A,B) showed the presence of neovascularisation of optic nerve head (NVD) and optical coherence tomography (OCT) of macula was essentially normal (figure 1A,B inset)

(A, B) Fundus photograph of right and left eyes, respectively, showing neovascularisation of optic nerve head (NVD) with inset showing normal optical coherence tomography at macula. (C) Late arteriovenous phase ultrawide field fundus fluorescein angiography (UW-FFA) of right eye showing NVD and an area of vascular staining with perivascular sheathing (red arrow), multiple microaneurysms, perivascular leakage and extensive peripheral capillary non-perfusion areas (yellow arrow). (D) An arterial phase UW-FFA of left eye showed delayed peripapillary choroidal filling and optic disc hypoperfusion (red arrow). Small white opacity temporal to fovea in (A) and just adjacent to disc in (B) was an artefact.
An ultrawide field fundus fluorescein angiography (UW-FFA) of both eyes revealed delayed arm to retina time of 56 s along with the presence of numerous microaneurysms, NVD, few areas of perivascular staining with minimal leakage, peripheral capillary non-perfusion areas (figure 1C) and delayed peripapillary choroidal filling (figure 1D) with optic disc hypoperfusion.
OCT angiography (OCTA) of the optic disc confirmed the presence of NVD in the optic nerve head slab of both eyes (figure 2A,B) along with peripapillary segmental flow void areas in choriocapillaries slab of both eyes using Image J software (figure 2C,D) which helped in diagnosing an anterior ischaemic optic neuropathy. Hence, a final diagnosis of bilateral stage 4 Takayasu retinopathy with anterior ischaemic optic neuropathy and ocular ischaemic syndrome was made.1–3 Panretinal photocoagulation was done in both eyes and subsequently she underwent bilateral carotid endarterectomy for carotid artery occlusion. At 2-month follow-up, IOP in both eyes was 14 mm Hg and her BCVA had improved to 20/40 and 20/60 in right and left eyes, respectively. Fundus examination showed pallor of optic nerve head secondary to ischaemic optic neuropathy along with regressing NVD (figure 3A,B) which was confirmed on OCTA (figure 3C,D).
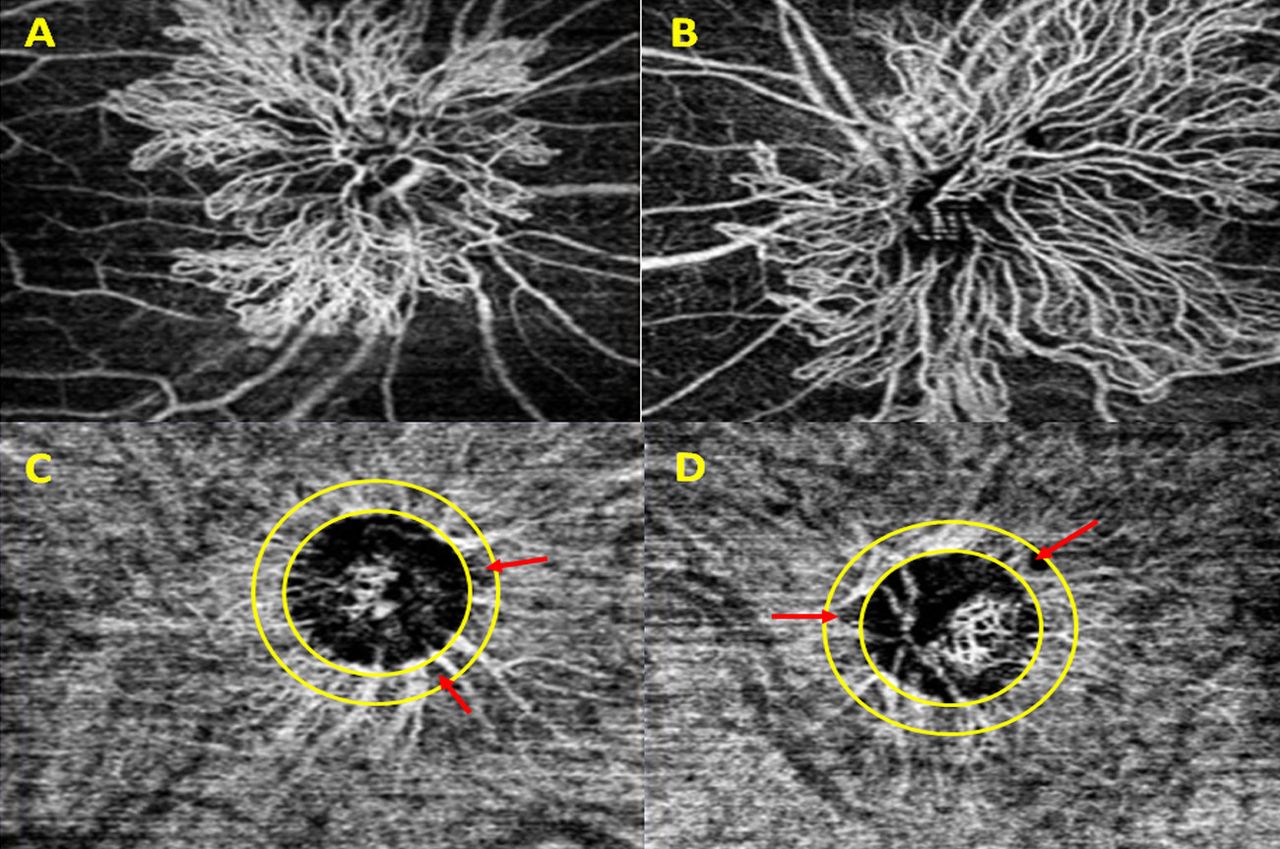
(A, B) Optical coherence tomography angiography (OCTA) at optic nerve head of right and left eyes, respectively, showing extensive florid neovascularisation of optic nerve head. (C, D) OCTA at choriocapillaries slab of right and left eyes, respectively, showing segmental peripapillary flow deficit areas (red arrow).

{kind=link}
{kind=link}
{kind=link}
(A, B) Fundus photograph of right and left eyes, respectively, showing pan retinal photocoagulation laser marks. (C, D) Optical coherence tomography angiography of optic nerve head demonstrating regressing neovascularisation of optic nerve head of right and left eyes, respectively.
Takayasu arteritis is a chronic granulomatous inflammatory arteritis involving mainly the large arteries of the body.4 Ocular manifestations are due to affection of the carotid arteries leading to improper perfusion of the ophthalmic artery. Ocular manifestations have been described by various groups ranging from involvement of retinal veins and occlusion of large arteries, microaneurysms, ischaemic optic neuropathies5 6 to complications like cataract, neovascularisation of the iris and retina leading to vitreous haemorrhage and neovascular glaucoma.7
Our case showed the presence of peripapillary flow deficit areas in OCTA which were evaluated using Image J software8 along with delayed peripapillary choroidal filling and optic disc hypoperfusion on UW-FFA9 which helped us in arriving at a diagnosis of an underlying ischaemic optic neuropathy.
To conclude Takayasu arteritis has a gamut of varied ocular manifestations with unexplained vision loss in some cases and multimodal imaging can help in arriving at correct diagnosis and treatment in such cases.
Patient’s perspective
I’m under regular follow-ups with my rheumatologist for Takayasu arteritis and I’m thankful to my rheumatologist for timely referral to ophthalmologist for this eye disease. Knowing the fact that I may have subnormal vision for rest of my life but I’m happy that further complications were prevented.
Learning points
Optical coherence tomography angiography (OCTA) can help in assessing peripapillary flow void areas and can help unveil an underlying anterior ischaemic optic neuropathy.
Multimodal imaging especially OCTA combined with fundus fluorescein angiography can be an useful tool in diagnosing anterior ischaemic optic neuropathy and ocular ischaemic syndrome in cases of Takayasu arteritis.
Footnotes
Contributors SR: writing manuscript, editing and review. MT: manuscript editing and review. AS: photography. AD: manuscript review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.