Article Text

Statistics from Altmetric.com
Description
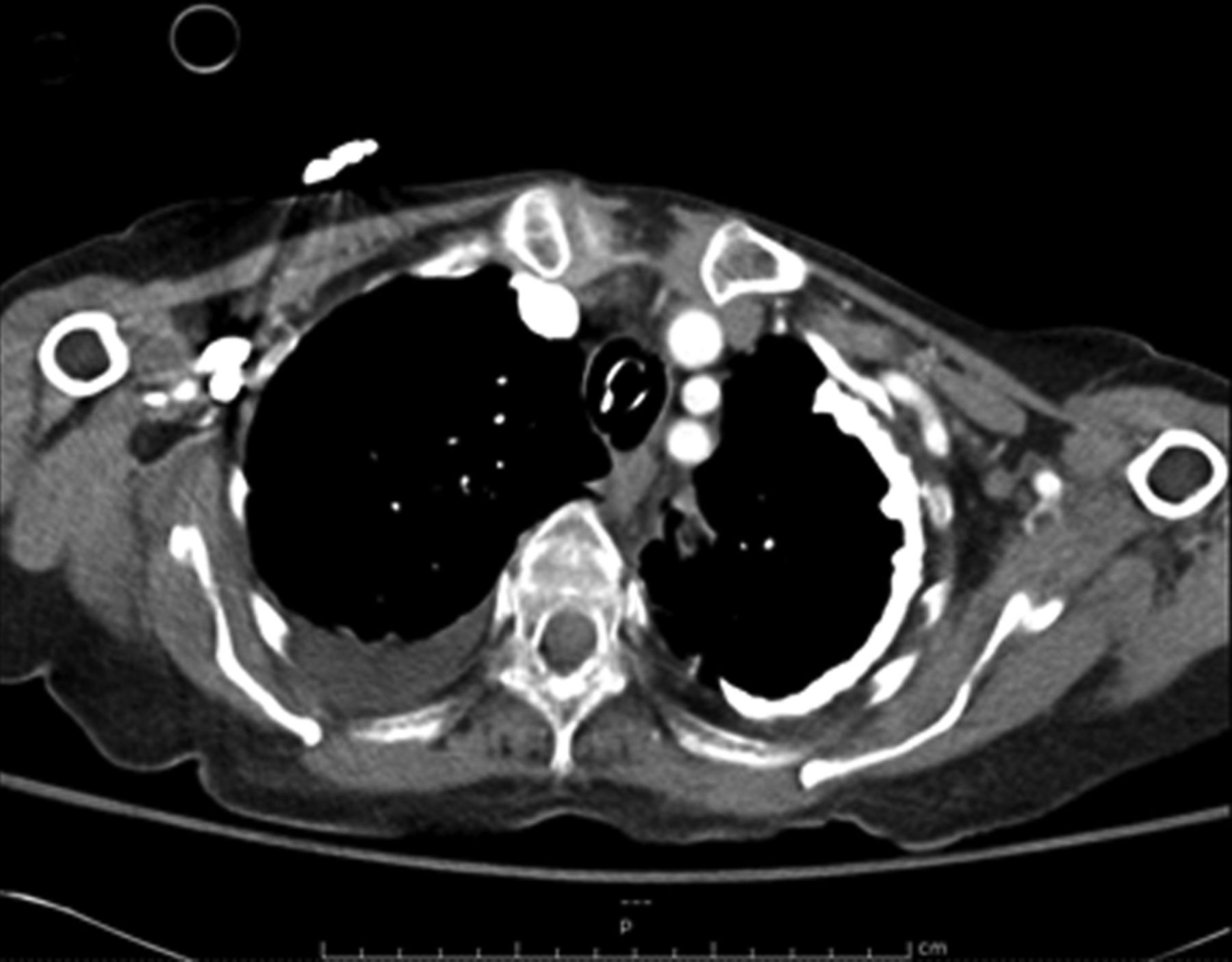
An 82-year-old Persian woman, with a history of pulmonary tuberculosis as a child, presented with gradual increasing dyspnoea. Her arterial blood gas showed severe respiratory acidosis and she was intubated. Her chest x-ray revealed a significant calcification encasing the majority of the left lung with a predilection towards the lung apex and pleural thickening which was redemonstrated on a subsequent chest CT (figures 1 and 2). She had normal renal function. Serum calcium and phosphorus were normal and she had no history of asbestos exposure. The patient had a hospital course complicated by gastrointestinal bleeding and pneumonia. The family elected comfort care and the patient died after prolonged hospitalisation.

A chest x-ray showing significant calcification encasing majority of the left lung with a predilection towards the lung apex with associated underlying pleural thickening.
{kind=link}
{kind=link}
A chest CT showing extensive left pleural calcifications and pleural thickening. The right-sided effusion was found to be transudative on thoracentesis.
Our patient had extensive pleural calcification secondary to old pulmonary tuberculosis. Late sequelae of tuberculous pleuritis include chronic persistent pleural effusion, empyema necessitatis, bronchopleural fistula, pleural malignancy, fibrothorax and pleural thickening which may be associated with extensive calcification.1
Other conditions such as haemothorax, empyema, talcosis, asbestosis and secondary hyperparathyroidism can result in pleural calcification as well.2
The distribution of pleural calcification can carry a diagnostic significance, for example, diaphragmatic pleural calcification is highly suggestive of asbestosis and unlikely to be caused by tuberculosis in which the pleural reaction is most commonly apical and asymmetric.2 ,3
Patients with diffuse pleural thickening should be closely monitored for the development of restrictive lung disease with serial pulmonary function tests. The main treatment focus is to treat the underlying disease. Pleural decortication in setting of extensive pleural calcification is of limited value specially with underlying parenchymal lung disease.
Learning points
-
Sequelae of a common disease can manifest itself much later in the course of life and can be missed if a thorough history is not obtained and corroborated with the physical examination findings and imaging.
-
Patient's history with regard to travel and/or residence is also essential since the pathological process in question may have been acquired in a totally different geographical location and its sequelae may or may not be very common in the area where it is diagnosed.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.