Article Text

Summary
Pectus excavatum is usually considered meaningless and without clinical significance. The following case may put a different complexion on the matter. A healthy 59-year-old male patient complained of progressive heart palpitations, fatigue and postural dyspnoea; bending over caused a clear increase of dyspnoea. At repeated examinations no overt abnormality or explanation was found, except a supraventricular arrhythmia and a nodal tachycardia. In the years to follow the symptoms led to considerable physical impairments. Finally, the patient himself, after searching the web, came up with a possible cause: his pectus excavatum. A lateral chest x-ray with the patient bending over and a lateral computed tomography of the thorax revealed an impression of the heart by the sternum. Ten years after the patient’s signs and symptoms first appeared, a modified Ravitch procedure was carried out, after which the physical condition of the patient improved rapidly.
Statistics from Altmetric.com
Background
Pectus excavatum, a deformity of the sternum and ribs caused by an unbalanced costochondral hypertrophy, is a congenital abnormality, with a prevalence of 1 per 1000 patients; it occurs mostly in boys and frequently more members in a family are affected.1,2 Pectus excavatum may be associated with connective tissue disorders such as Marfan and Ehlers–Danlos syndrome.3 Pectus excavatum is commonly considered to be an incidental finding without clinical significance. It is usually found at physical examination or as a phenomenon reported in radiographic procedures. In the majority of cases it is ‘diagnosed’ in young patients. Signs are usually cosmetic, although severe cases may notice difficulties in breathing. The deformity of the chest wall is often noticed at birth, but becomes more pronounced in adolescents. After the age of 18 years, the deformity usually does not change anymore. Pectus excavatum is considered to be solely a cosmetic problem, despite the fact that there may be a considerable compression and relocation of thoracic organs. It can, however, lead to serious cardiac symptoms.
What is much less known is that, as patients get older, this abnormality may also lead to serious signs and symptoms, some of them leading to considerable physical impairments. In the literature there are very few papers in the specific specialist journals that have addressed this issue.2–7 These articles suggest that pectus excavatum can indeed cause severe symptoms in elderly and that surgery can result in complete recovery from symptoms.
The current case report describes the possible consequences of pectus excavatum and is presented to raise awareness that pectus excavatum is not always as harmless as it is considered to be. Especially for general practice, this is a relevant and new insight as most patients with pectus excavatum are usually managed within primary care.
Case presentation
A 59-year-old male physically active patient (former general practitioner) contacted his GP complaining of palpitations and shortness of breath after exercise. A routine electrocardiogram (ECG) revealed ventricular extra systoles and a paroxysmal nodal tachycardia (heart rate 220/min). A cardiologist and lung specialist confirmed these findings, but despite detailed further analysis no underlying disease was found. Drug treatment with sotalol and verapamil had only temporary effects, and physical exercise became increasingly problematic.
Six years later the cardiologist and lung specialist repeated their analyses. Except for occasional (supra)ventricular tachycardia measured in a Holter registration, no abnormalities were found. The dissatisfactory diagnosis was: ventricular extrasystoles, nodal tachycardia, and congestive heart failure of unknown origin. Meanwhile, the patient himself noticed that dyspnoea not only occurred after exercise but also postprandially, and depended on posture (bending over, in particular).
In the following years, the symptoms increased and the patient became orthopnoeic. He tried to cope with his impairments by a series of measures such as eating smaller amounts of food, reducing exercise, etc. Climbing stairs without resting became impossible.
In a desperate attempt to seek relief of discomfort, the patient started using glyceryl trinitrate (GTN, nitroglycerine), resulting in a dramatic but unfortunately only temporary improvement. Angiography was completely normal, the effect of the GTN could not be explained. So, 8 years after the first onset of symptoms, an explanation for the patient’s condition was still lacking.
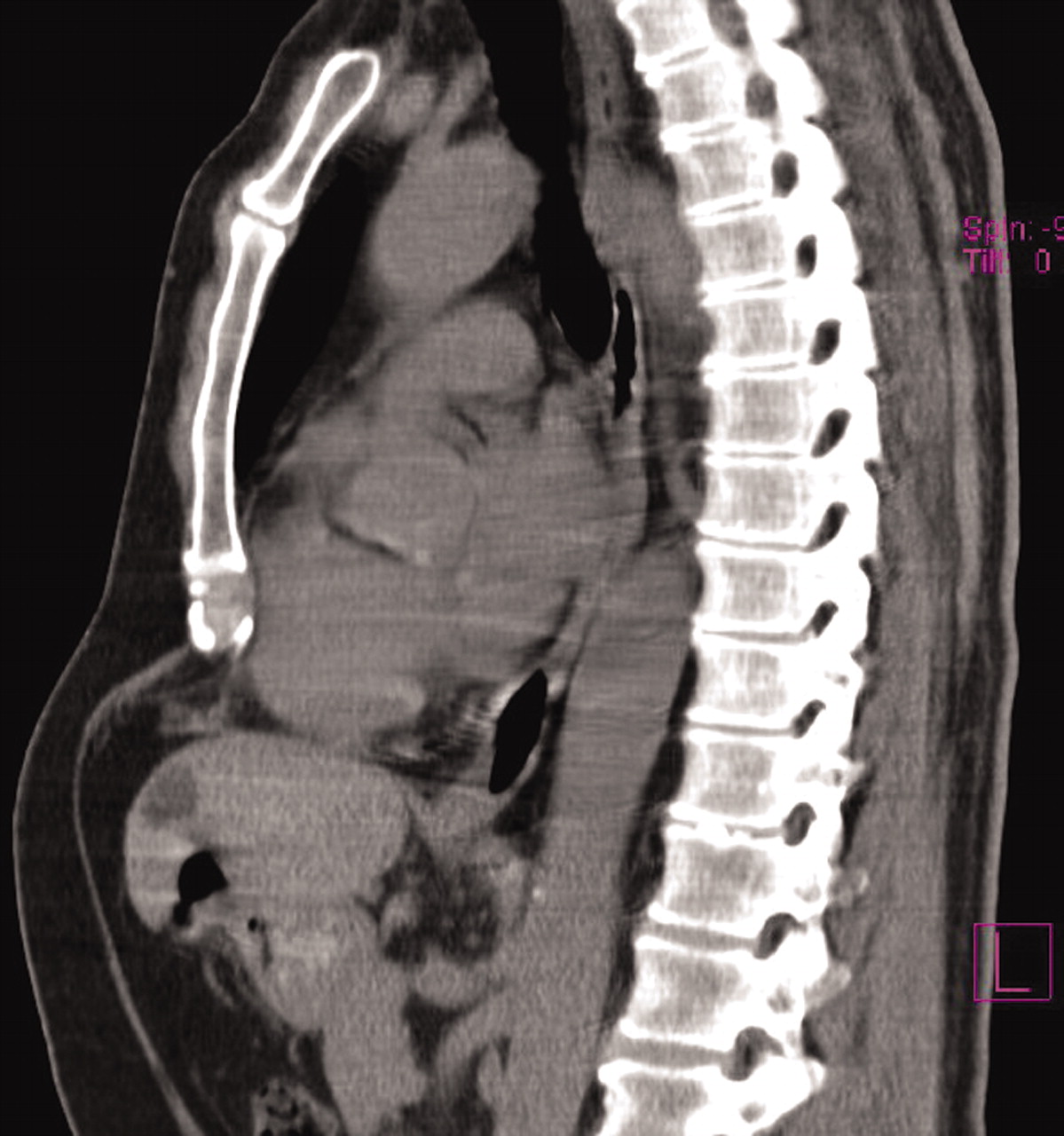
After a web search, the patient came up with an explanation: his pectus excavatum (fig 1). Initially, reactions were sceptic but the patient was ultimately referred to a thoracic surgeon with expertise in treating pectus excavatum.
{kind=link}
Computed tomography scan of patient’s chest wall deformity.
Outcome and follow-up
One month later the patient underwent surgery, a modified Ravitch procedure. The original Ravitch operation was described in 1949. Most surgeons now use less invasive modifications which include bilateral resection of the costal cartilages, sternal remodelling and a steel sternal support, through a 8–10 cm submammary skin incision.8,9 Soon thereafter, the patient was almost completely relieved from fatigue and shortness of breath. After 3 months, heavy physical exercise was possible again, with only minor arrhythmia.
Discussion
Based on the previous case history, suggesting a causal relation between pectus excavatum and symptoms such as fatigue, shortness of breath and palpitations, and impressions from the literature, pectus excavatum may not always be as harmless as it seems. Especially in the elderly, the symptoms may easily be confused with cardiac problems such as heart failure. From a practical viewpoint this means that detection of a pectus excavatum when examining the patient should not be neglected and should be considered as a possible explanation for the following symptoms: shortness of breath and/or palpitations (especially after exercise or when postural), chronic fatigue, and, on ECG, ventricular extra systoles and/or atrioventricular nodal tachycardia in the absence of other adequate explanations.
This is especially relevant as in the case of symptomatic pectus excavatum in seniors (SPES) there are treatment options allowing complete recovery.
There are no data on the prevalence of pectus excavatum in elderly patients, but there is reason to believe that the prevalence in elderly patients equals that in children. As the appearance of symptoms may increase with age, it would be interesting to know the prevalence of symptoms among elderly patients with pectus excavatum. Until now, data on this have been lacking and further research on the prevalence and the pre-test probability of signs and symptoms is recommended.
Learning points
-
Pectus excavatum may not be as harmless as it seems.
-
Pectus excavatum may become symptomatic with increasing age
-
In elderly patients with dyspnoea, fatigue and palpitations, pectus excavatum may be a cause in the absence of another explanation.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication