Article Text

Statistics from Altmetric.com
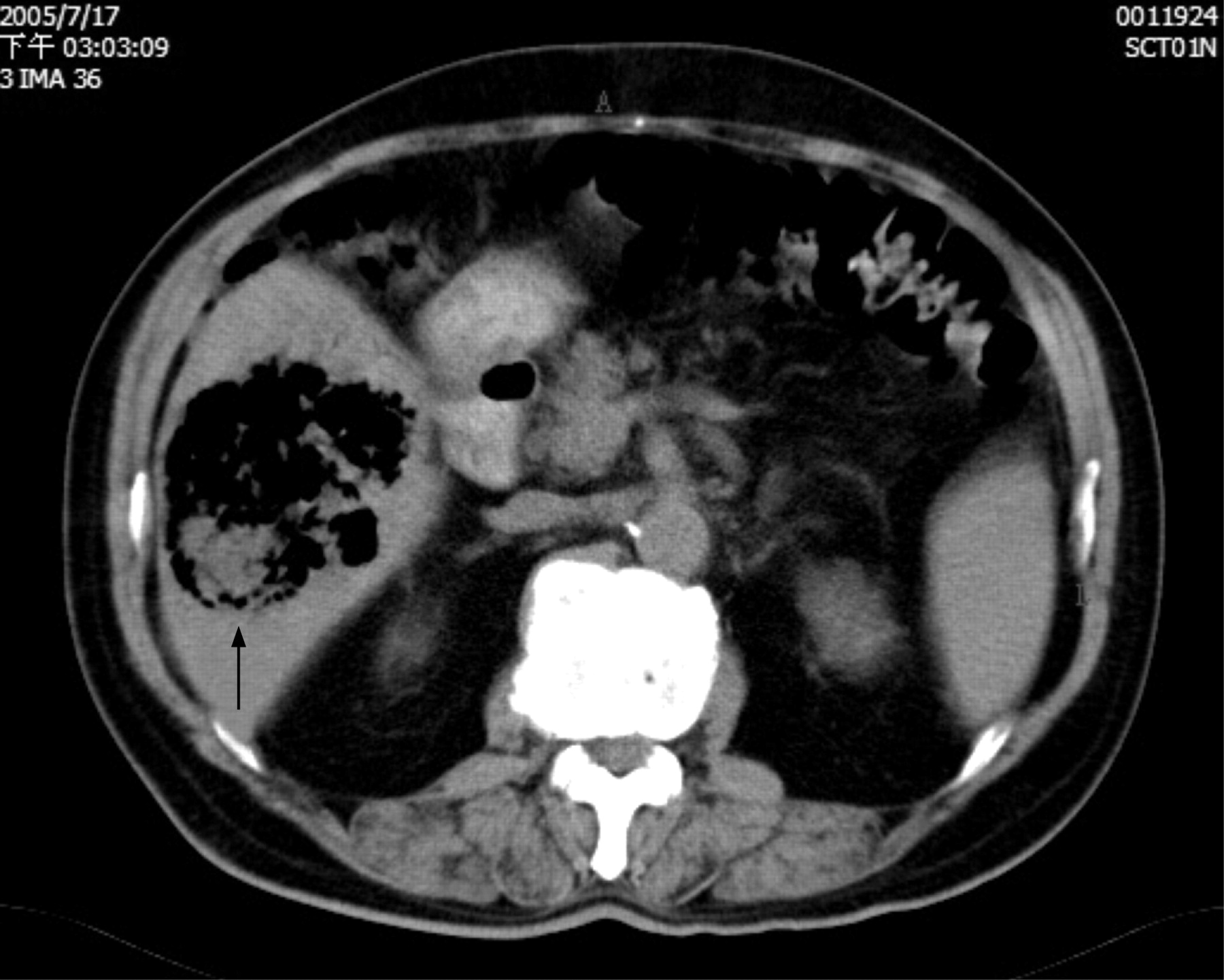
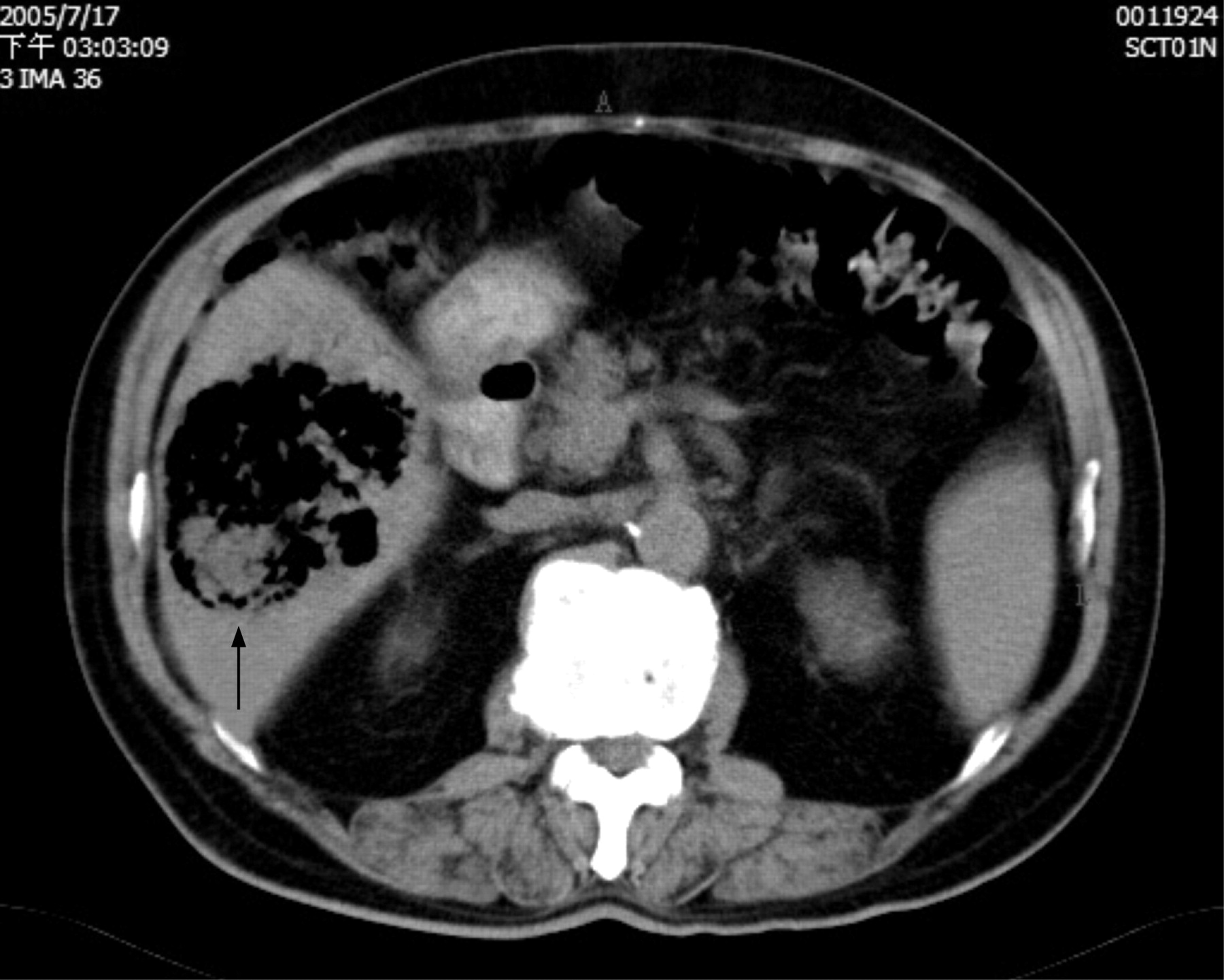
A 71-year-old man presented to the emergency department with fever and chill for 3 days. He had type 2 diabetes mellitus for 2 years. On arrival, his vital signs were stable and his physical examination was unremarkable except for mild right upper quadrant tenderness. The patient’s white blood cell count was 18580/mm3; aspartate aminotransferase and alanine aminotransferase were 360 IU/l (normal range 0–38) and 329 IU/l (normal range 0–44), respectively. Stool-like material accumulating in the right upper quadrant was disclosed on the plain kidney–ureter–bladder (KUB) film (arrow, fig 1). A non-contrast abdominal computed tomography (CT) scan was performed which revealed a huge gas containing liver abscess (arrow, fig 2). CT guided percutaneous catheter drainage was carried out soon after the diagnosis of liver abscess. Both the abscess and blood culture yielded Klebsiella pneumoniae.

Stool-like material accumulates in the right upper region of abdomen on plain kidney–ureter–bladder (KUB) film (arrow).
{kind=link}
{kind=link}
A non-contrast abdominal computed tomography scan shows a huge gas containing liver abscess (arrow).
Pyogenic liver abscess is usually a polymicrobial infection in western countries. In Taiwan, however, liver abscess has usually been caused by K pneumoniae, especially in patients with diabetes.1 This condition has also been reported in western countries, representing a global emerging infection.2 In our case, the lesion on the right upper quadrant of the KUB film could be mistaken for stool. However, the patient presented with symptoms and signs of infection. This abnormal lesion shown on KUB film should alert physicians to look for possible infection foci. Because liver abscess could present as gas forming lesions, particular among patients with diabetes,3 physicians should therefore consider such a manifestation of liver abscess on KUB film.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.