Article Text

Statistics from Altmetric.com
Until the 1950s, cardiac tumours were merely a curiosity. Diagnosis was academic and outlook poor. With the advent of cardiopulmonary bypass, however, surgical management became possible, particularly of intracavity tumours. More recently, the development of echocardiography, compututed tomography, and magnetic resonance imaging has contributed greatly to the process of preoperative diagnosis.
Epidemiology and nomenclature
Primary cardiac tumours are rare, with a necropsy incidence of 0.05%.1 Secondary deposits are seen more frequently, in 1% of postmortem examinations, but usually in the setting of widely disseminated malignancy.2 The relative incidence of presentation is shown in table 1, and demonstrates that atrial myxoma is by far the most common primary cardiac tumour in adults, and rhabdomyosarcoma is the most common in children. A quarter of all cardiac tumours are malignant, the majority of which are angiosarcomas or rhabdomyosarcomas.
Approximate incidence of benign tumours of the heart in adults and children
General clinical features
Cardiac tumours are diverse in clinical presentation, and atrial myxomas in particular may cause systemic symptoms mimicking collagen vascular disease, malignancy or infective endocarditis. There are several clinical features, however, that are seen commonly with many cardiac tumours:
Embolisation—This occurs frequently. Either the tumour itself, or adherent thrombus may dislodge and migrate; hence the age old aphorism that all retrieved emboli should be examined histologically. Multiple small emboli may mimic vasculitis or endocarditis, while larger fragments may lead to cerebrovascular events. Right sided tumours naturally embolise to the lungs producing pleuritic symptoms and possibly right heart failure.
Obstruction—Atrial tumours, once they are large enough, may result in obstruction of atrioventricular valvar flow, and, in particular, may mimic valvar stenosis. Symptoms are often markedly paradoxical and may relate to body positions. Ventricular tumours, though in general less frequent, may obstruct outflow tracts leading to chest pain, breathlessness or syncope.
Arrhythmias—Intramyocardial and intracavity tumours may both affect cardiac rhythm, either through direct infiltration of the conduction tissue, or through irritation of the myocardium itself. Atrioventricular block and ventricular tachycardia are not infrequently seen, and the initial presentation may be with sudden death. The presence of serious ventricular arrhythmias should always lead to a search for structural heart disease and very infrequently a tumour may be found.
Epidemiology and presentation
Primary cardiac tumours are rare
The most common primary cardiac tumour is the atrial myxoma
A quarter of primary cardiac tumours are malignant, the vast majority being sarcomas
Embolisation, obstruction, and arrhythmogenesis are the chief modes of presentation
Surgically retrieved emboli should be examined histologically
Sudden death is not uncommon
Myxoma
Atrial myxoma is the most common cardiac tumour, comprising 50% of tumours. Occurring more commonly in women, myxomas are usually diagnosed between the ages of 50 and 70 years, 90% are left atrial, and 90% are solitary. Sometimes myxomas are familial, in which case they are seen in younger patients. Facial freckling and endocrine adenomas are frequent. The tumours are much more frequently multiple whereas the sporadic cases are almost all single and atrial. Under these circumstances, screening of first degree relatives should be undertaken. Multiple acronyms have been proposed for such syndromes. These include LAMB (lentigines, atrial myxoma, mucocutaneous myxoma, and blue naevi) and NAME (naevi, atrial myxoma, myxoid neurofibromata, and ephelides). Recent nomenclature, however, suggests that they should be brought together under a broader category of Carney complex, named after the physician who first described the familial nature of this disorder.3 A recent study of four relatives with the Carney complex suggests that the disease is caused by a gene deletion at the 17q2 locus.
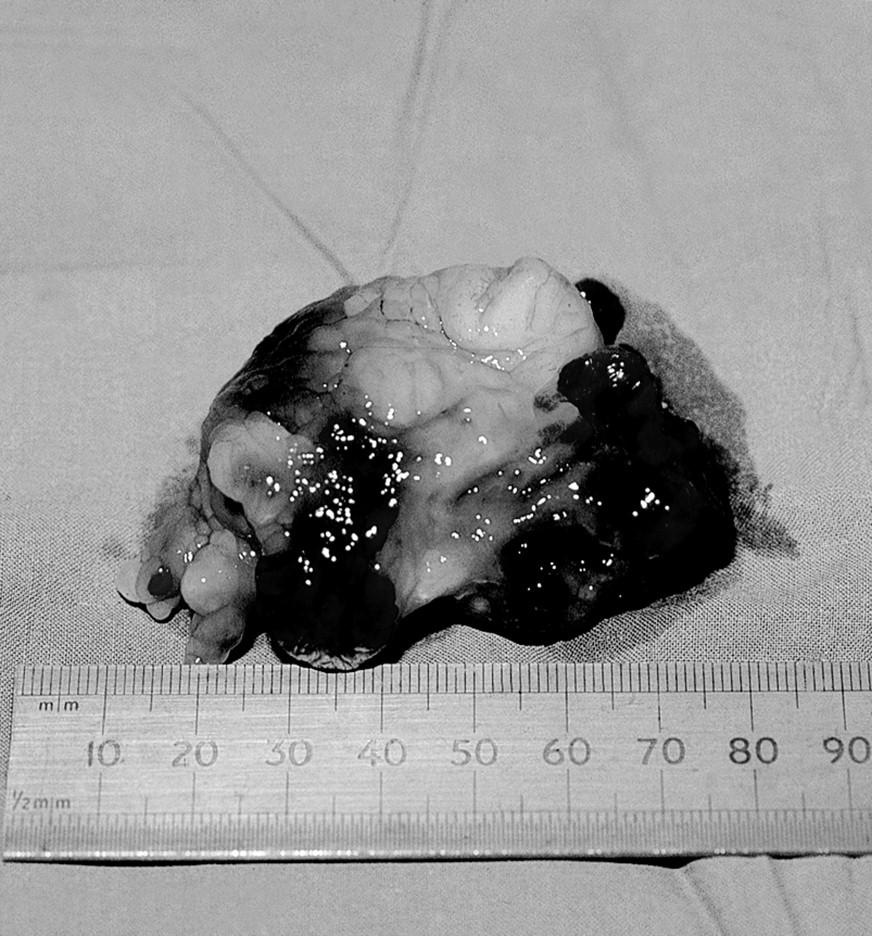
The cell of origin of the myxoma is not known. Macroscopically they appear irregular, shiny and coloured (fig 1). Occasionally they are calcified. Their pedunculated nature means that the tumour may be very mobile and may obstruct a valve orifice (fig 2). The majority of myxomas are attached to the left atrial septum around the fossa ovalis, often with a component protruding through the atrial septum to the right side (fig3).

Macroscopic specimen of an atrial myxoma. Note the irregular, heterogenous, and polypoid nature of the tumour.

Transoesophageal echocardiogram showing a left atrial myxoma prolapsing across and obstructing the mitral valve.

Transoesophageal echocardiogram (180° therefore left-to-right inversion) showing a left atrial myxoma, again obstructing the mitral valve orifice but also spreading across the fossa ovalis into the right atrium.
Clinical features
Clinical manifestations are legion, both cardiac and systemic. Symptoms include breathlessness, fever, weight loss, syncope, haemoptysis, and sudden death. Emboli both of tumour fragments and thrombus from the tumour surface may present in a dramatic fashion. Multiple systemic emboli may imitate vasculitis and infective endocarditis. The features may mimic systemic infection with cachexia, fever, arthralgias, and raised inflammatory markers. Very occasionally patients with transient ischaemic attacks or stroke are found to have an isolated myxoma only diagnosed by echocardiography. Right sided tumours embolising to the lungs result in pulmonary hypertension. Physical signs are also very variable and include clubbing, rash, and other features of infection and inflammation. Murmurs are frequently present, as is evidence of pulmonary hypertension, right sided cardiac failure, and pulmonary embolisation. Anaemia, raised acute phase reactants, and erythrocyte sedimentation rate are frequently present. Less frequently, the characteristic “tumour plop” may be detected. This is heard as a loud but rather dull sound as the tumour prolapses into the left ventricle, and may be confused with a third heart sound. Occasionally patients undergoing routine echocardiography for other indications are found to have a myxoma; despite the lack of clinical symptoms and signs they should have a surgical resection.
Diagnosis
Diagnosis depends on a high index of suspicion and can almost always be made by echocardiography. Both transthoracic and transoesophageal imaging should demonstrate a tumour and its relation to the atrial septum. If the exact origin cannot be seen, often an echo of increased amplitude may be visualised or the traction on the atrial septum may be noted as the tumour prolapses through the mitral valve. Differentiation of myxoma from valvar vegetation and, more importantly, from atrial thrombus is important. Usually the echocardiographic appearance of a myxoma is quite distinctive. In addition to the characteristic location and pedicle, myxomas are heterogenous and may have small lucencies. Thrombus is usually homogenous in appearance (though occasionally a liquefied centre may give rise to reduced echo amplitude), and usually arises from the left atrial appendage. Diagnostic confusion may exist when the myxoma arises from the left atrial appendage, as it does in 5% of cases. In this situation, the clinical setting of the illness and corroborating features should help to distinguish myxoma from thrombus. Occasionally, however, the two may be impossible to distinguish on the basis of clinical and imaging criteria and a surgical approach may be required in the absence of a clear diagnosis. Alternatively, if the mass is small it has been recommended that a period of oral anticoagulation may help in differential diagnosis. Right atrial myxomas are relatively rare, but may cause diagnostic confusion as they may be mistaken for embolised or in situ thrombus. In these cases, it is important to look carefully to see if the mass is growing through the foramen ovale. Where diagnostic confusion persists after echocardiography, magnetic resonance imaging may prove helpful.4
Myxoma
90% are left atrial
90% are solitary
Associated facial freckling should raise the possibility of the Carney complex, in which case family members should be screened
The clinical features may mimic infective endocarditis, vasculitis or other inflammatory disorders
Differentiation from intra-atrial thrombus is important
Surgical resection is advisable as soon as possible after diagnosis, as the risk of embolisation is high.
Recurrence is possible, and therefore long term echocardiographic follow up is recommended
Management
The method of choice for treating atrial myxomas is early surgical resection on cardiopulmonary bypass. These tumours are histologically benign but patients may die from obstruction, distal embolisation or rhythm disorders. Dislodgement of tumour fragments can be a significant risk during operative resection, and to reduce this possibility manipulation of the heart is reduced to a minimum. Atrial myxomas may occasionally recur, either due to a second tumour origin, failure to demonstrate a pre-existing tumour focus or incomplete excision. Surgical survival following resection is excellent, but long term follow up is usually recommended, with echocardiography, to exclude development of a new tumour. However, the rate of reoccurrence is now so low most patients could be safely discharged.
Other benign primary cardiac tumours
Papillary fibroelastoma
These small tumours of the valve apparatus are often incidental postmortem findings. With the developments in echocardiographic imaging, they may be visualised during life, when they may be mistaken for valvar vegetations (fig 4). Until recently these tumours were considered to be benign and insignificant, but recent postmortem studies have demonstrated a high incidence of embolisation to cerebral and coronary arteries, and surgical resection is now considered more appropriate.5 The “sea anemone” appearance, with a short attaching pedicle, is typical. Microscopically, each frond is formed of a central fibroelastic core, an overlying myxomatous layer, and an endothelial covering. Their pathological origin, however, remains elusive.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transoesophageal images of an aortic papillary fibroelastoma in (left) longitudinal long axis and (right) short axis transverse views.
Rhabdomyoma
This intramyocardial tumour is the most frequent cardiac neoplasm of childhood, and is almost always multiple and ventricular. They may be seen by echocardiography as a pedunculated mass which may obstruct ventricular inflow or outflow. The majority of children with cardiac rhabdomyomas also have tuberous sclerosis.6 Spontaneous tumour resolution is common, and treatment is therefore usually conservative. Life threatening complications are unusual, but occasionally surgical resection is necessary.7
Lipoma
These encapsulated tumours are usually subepicardial and asymptomatic. Rarely they may become large and cause arrhythmias, including atrioventricular block. Occasionally they may extend into the left atrial cavity but tend to avoid the fossa ovalis. If diagnostic confusion exists, magnetic resonance imaging is characteristic.8 Lipomatous hypertrophy of the interatrial septum is a separate, non-neoplastic condition, usually found in obese patients, in which the atrial septum is heavily infiltrated with adiposity. This is seen by ultrasound as a very thickened atrial septum (2–3 cm) with low echo density. If atrial tachyarrhythmias are problematic, weight loss may be beneficial.
Fibroma
Cardiac fibromas are low grade connective tissue tumours which are usually intraventricular and occur principally in childhood. Firm, grey-white masses, they range from 1–10 cm in diameter. The echocardiographic appearance is of discrete, often obstructive masses. Grossly they appear sharply demarcated, with multiple foci of calcification which may aid diagnosis as they are often well seen by fluoroscopy. Located chiefly in the interventricular septum, these tumours interfere with the conduction system. Ventricular arrhythmic symptoms are common and sudden death is not rare. Surgical excision is sometimes possible, but transplantation has also been advocated.
Angioma
These tumours are extremely rare, and occur principally in the interventricular septum. They are visualised as subendocardial nodules, usually 2–4 cm in diameter. Coronary angiography may reveal a characteristic “tumour blush”. Microscopically, they are classified as capillary, cavernous, intramuscular or haemangioendotheliomatous, though this does not seem to influence prognosis. Total surgical excision is not usually feasible because of the highly vascular nature of the tumour. Ventricular tachycardia and cardiac tamponade may intervene.
Other benign primary cardiac tumours
Papillary fibroelastomas have a high incidence of embolisation—consideration should be given to surgical resection
Rhabdomyoma is the most common cardiac neoplasm of childhood, often seen in association with tuberous sclerosis
Lipomas are usually asymptomatic
Lipomatous hypertrophy of the interatrial septum should not be mistaken for intracardiac tumour
Malignant primary cardiac tumours
Approximately a quarter of all cardiac tumours exhibit some features of malignancy or behave in a malignant way; 95% of these are sarcomas,9 the other 5% being lymphomas. Sarcomas are common between the third and fifth decades of life and most frequently affect the right atrium. They display a wide variety of morphologies owing to their mesenchymal origin. The clinical course is usually rapidly progressive, with death occurring as a result of widespread local infiltration, intracavity obstruction or metastases.
Angiosarcomas
These tumours occur more commonly in men, and almost exclusively in the right atrium. Clinical features include congestive cardiac failure, pericardial effusion, and pleuritic chest pain. Occasionally non-specific signs of disseminated malignancy, such as fever, weight loss and lassitude appear before signs of cardiac involvement. Echocardiography usually shows a broad based right atrial mass near the inferior vena cava. Epicardial, endocardial or intracavity extension is common and local spread of the tumour to pleura or mediastinum is often found. Pulmonary metastases are frequent and survival after diagnosis rarely exceeds six months.10 Adjuvant chemotherapy seems to have little to offer at present.
Rhabdomyosarcomas
These tumours, the second most common primary sarcomas of the heart, are also more common in males, but may involve any cardiac chamber. Non-specific symptoms of malignancy are the rule, though pleuro-pericardial symptoms and distal embolisation may occur. Arrhythmias and obstructive symptoms may develop and raise the suspicion of a primary cardiac lesion. In contrast to angiosarcoma, diffuse pericardial involvement is not a feature and the tumour only rarely infiltrates beyond the parietal pericardium. Response to chemotherapy has been reported, and tumour bulk may be followed sequentially with magnetic resonance imaging,11 but survival remains poor.
Others
Fibrosarcomas, histiocytomas, and lymphomas constitute the remainder of primary malignant cardiac tumours. Fibrosarcomas are malignant mesenchymal tumours which are primarily fibroblastic in origin, and occur with equal frequency on left and right sides of the heart. Firm, grey-white and nodular, they are often multiple and may invade the cardiac chambers and the pericardium. Survival is poor. Malignant fibrous histiocytomas are differentiated from fibrosarcomas by the typical whorled pattern of spindle cells on histology, but clinically behave in much the same way as fibrosarcomas.
Primary lymphomas must, by definition, involve only the heart and/or pericardium. They are rare, though in the last 20 years the incidence has been rising as they are seen as part of the acquired immunodeficiency syndrome12 and in transplant recipients on immunosuppressive regimes. Lymphomas may go unrecognised as the chief presentation is with intractable heart failure. Treatment involves surgical resection and radiotherapy, but again with limited success.
Malignant primary cardiac tumours
The majority of malignant primary cardiac tumours are sarcomas, usually angiosarcomas or rhabdomyosarcomas
Most primary cardiac tumours are right atrial in location
The incidence of primary intracardiac lymphomas is increasing—they are seen as part of the acquired immunodeficiency syndrome
Treatment is rarely curative
Secondary cardiac tumours
Secondary cardiac tumours are usually epicardial and asymptomatic
Metastasis is rarely limited solely to the heart
Pericardial effusion is common
Melanoma, leukaemia, and lymphoma are most commonly associated with metastasis to the heart
Secondary cardiac tumours
Secondary cardiac tumours may be epicardial, myocardial or endocardial, but the vast majority are epicardial. With an incidence of up to 1% at necropsy, metastatic deposits to the heart are more than 20 times more common than are primary tumours.2 ,13Metastasis is rarely limited solely to the heart. The development of tachycardia, arrhythmias, cardiomegaly or heart failure in a patient with carcinoma should raise the suspicion of cardiac metastases. Rarely, cardiac involvement may be the first clinical feature of malignancy, and when this is the case, the presentation is usually with a large pericardial effusion or incipient cardiac tamponade. Metastases to the heart are, however, clinically silent in 90% of cases.
Local infiltration
Carcinoma of the lung or breast may spread by local infiltration to the pericardium, leading usually to pericardial effusion. Alternatively, carcinoma of the lung may invade the pulmonary veins and grow into the left atrium, occasionally causing symptoms as a result of mitral valve obstruction. Similarly, renal cell carcinoma has a tendency to invade the inferior vena cava, and may embolise to the right atrium, or may even grow as far as the heart.
Metastasis
For reasons which are not clear, melanoma has a particular predilection for metastasising to the heart. Half of all cases of disseminated melanoma will have cardiac deposits at necropsy,14 and these tend to affect all four chambers of the heart. Leukaemias commonly invade the heart. Leukaemic infiltration between myocardial cells and sometimes larger deposits may be found. Pericardial effusion is sometimes a feature, in which case the fluid is usually haemorrhagic. Lymphomas similarly metastasise to the heart with regularity, forming discrete intramyocardial masses which are usually clinically silent.