

To the Editor:
Relapsing polychondritis (RP) is a rare multisystem disease1 for which the etiopathogenesis is probably autoimmune. RP predominantly affects middle-aged Caucasians1, but it has been reported in 31 children and adolescents under 18 years of age1–3. It is mainly characterized by recurrent destructive inflammatory lesions of cartilaginous structures and proteoglycan-rich tissues1,3 such as outer and inner ears, nose, the laryngotracheobronchial tree, hyaline cartilage of joints, eyes, heart, and blood vessels; kidneys and skin may also be involved. We describe a rare and unique childhood articular manifestation of RP.
A 4-year-old girl of African descent was diagnosed with RP after a second episode of left-ear chondritis. Conjunctivitis and arthritis began 14 months later, involving proximal interphalangeal (PIP) joints, wrists, ankles, and knees. She developed a chronic arthritis course with some episodic flares. Nasal chondritis started 2 years later. Laboratory tests showed negative antinuclear antibody and rheumatoid factor, and during flares a moderate to high erythrocyte sedimentation rate, leukocytosis, and thrombocytosis. At the age of 10 years, she presented with enlargement of distal forearms and legs (Figure 1A) associated with peculiar radiological changes around the growth plate: metaphyseal widening and irregularities in the distal epiphysis of the radius, tibias, and fibulas (Figure 1B). Magnetic resonance imaging (MRI) showed edema in the tarsal bones and also in the metaphyseal regions of metatarsal bones and irregularities in the distal epiphysis of tibia, fibulas, and radius (Figures 1C, 1D).A biopsy performed in the distal growth plate of the radius revealed a loss of basophilic staining, inflammatory infiltrates, decreased number and pyknosis of chondrocytes, in addition to areas of growth cartilage replacement with fibroblastic granulation tissue.
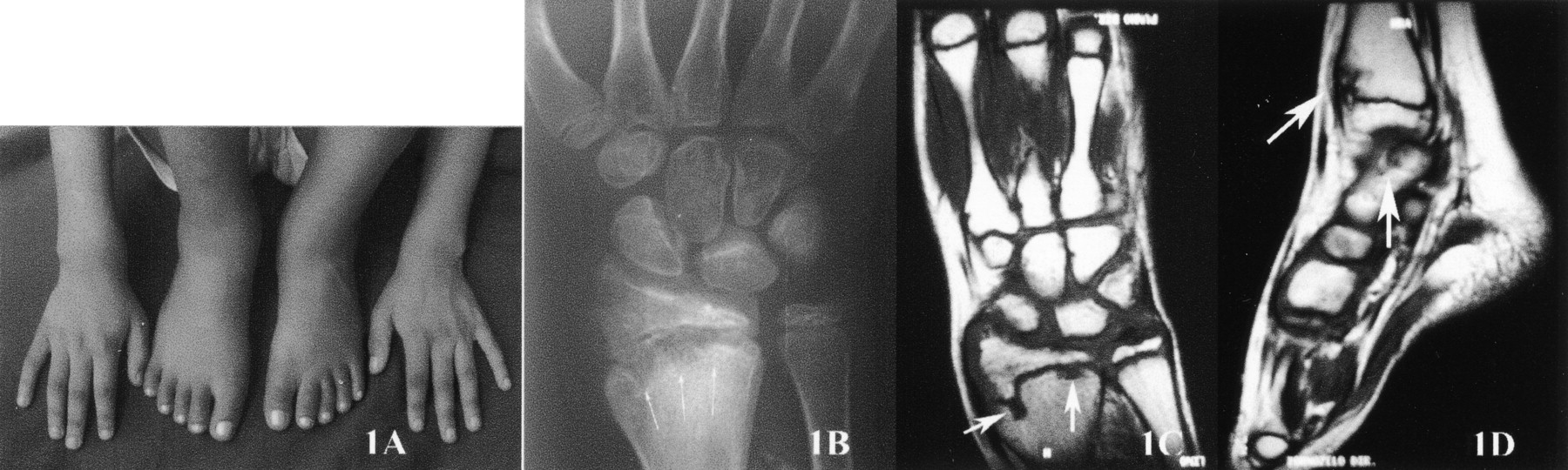
The patient at age 10 years. A. Widening of wrists and ankles; B. conventional radiograph of the right wrist shows metaphyseal widening and irregularities in the distal growth plate of the radius; C. coronal T1-weighted MRI of right wrist shows irregularity of the distal physis and epiphysis of the radius; D. sagittal T1-weighted MRI of the right ankle demonstrates, in the tibia, irregularity of the distal physis and anterior portion of the metaphysis, with some marrow edema. Edema of the navicular bone can also be seen.
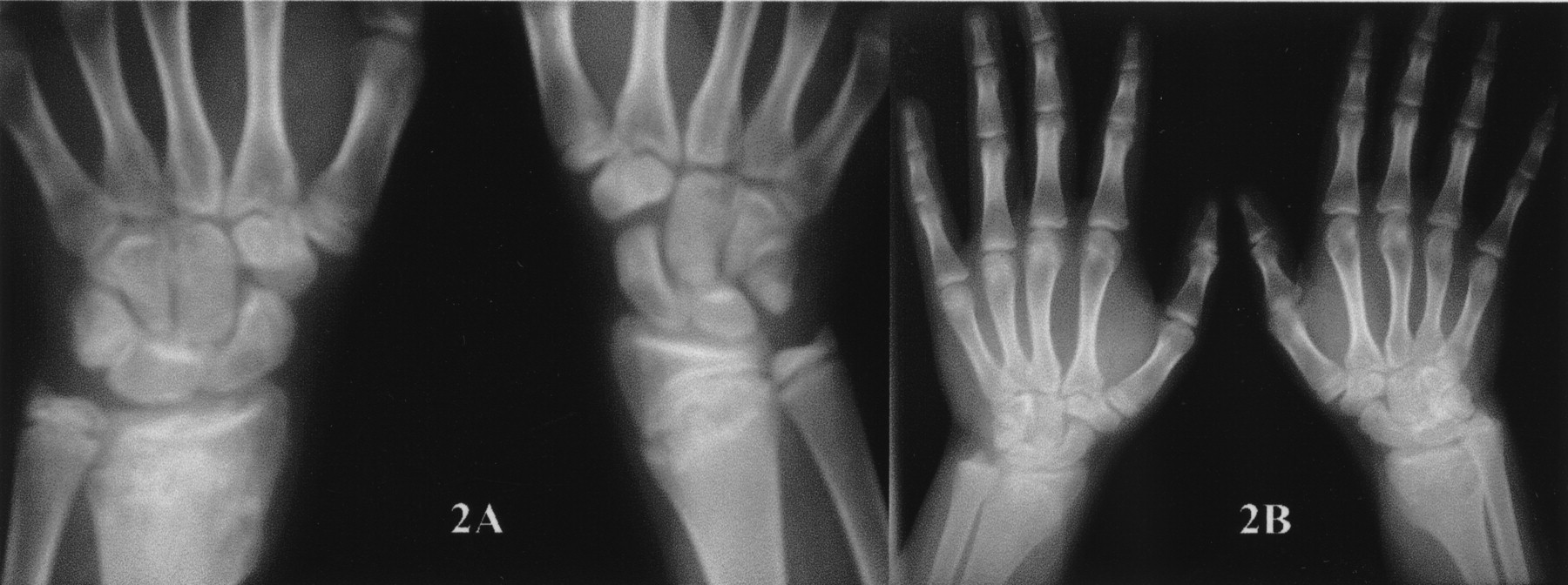
During 10 years of follow-up, no other organ has been involved (including airways) and she has been treated with corticosteroids, cyclosporine, azathioprine, infliximab, and recently with etanercept, which have yielded partial responses. There have been persistent bilateral deforming ear chondritis, deformities of the distal epiphysis, and laboratory markers of inflammation. However, it should be noted that linear growth and functional ability were not impaired, and also that erosive radiological changes resolved after epiphyseal fusion (Figures 2A, 2B).

Conventional radiographs at age 14 years (A) and 16 years (B) show that erosive radiological changes have not affected epiphyseal growth and fusion.
Articular manifestations (arthralgia, arthritis, and costochondritis) may occur in 70%–80% of adult and pediatric patients1–3. The most common pattern is episodic, asymmetric, nonerosive, nondeforming peripheral arthritis, lasting for weeks or months, commonly affecting ankles, wrists, PIP joints, metacarpophalangeal joints, elbows, and metatarsophalangeal joints3–5. Plain radiographs, in the absence of an associated disease, classically show only juxtaarticular osteopenia and minor uniform joint space narrowing, typically without erosive changes or deformities6,7. However, in this case, arthritis was persistent and destructive, with widening of distal forearms and legs, in addition to radiological and histopathological changes in the distal growth plate of the radius, fibulas, and tibias. There is a somewhat similar report8 in an 8-year-old boy, who developed a chronic polyarthritis with roentgenographic changes described as metaphyseal radiolucent defects of ulnas, radius, fibulas, and tibia, and also irregularities in the ossification centers of the fibulas, metacarpals, and proximal phalanges. Those rare articular and radiological findings may be considered unique to childhood RP.








{kind=link}
{kind=link}