Investigation and management of chronic dysphagia
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7386.433 (Published 22 February 2003) Cite this as: BMJ 2003;326:433
- Paula Leslie, dysphagia research speech and language therapist (paula.leslie{at}ncl.ac.uk),
- Paul N Carding, senior lecturer in voice pathology,
- Janet A Wilson, professor of otolaryngology and head and neck surgery
- Correspondence to: P Leslie
Dysphagia is an impairment of swallowing that may involve any structures from the lips to the gastric cardia. Causes include a wide variety of acute cerebral conditions, progressive disorders, and trauma, disease, or surgery to the oro-pharyngo-oesophageal tract (box 1). Department of Health figures for 2001–2 record more than 23 000 primary diagnoses of dysphagia in England and Wales, associated with almost 76 000 bed days in hospital.1 Even these figures do not adequately reflect the substantial healthcare costs of dysphagia.2 The aim of this review is to summarise the incidence, causes, and risks of dysphagia and to provide a detailed update on investigation and management, including the need for a multidisciplinary approach.
Summary points
Dysphagia is impairment of swallowing involving any structures of the upper gastrointestinal tract from the lips to the lower oesophageal sphincter
Causes of dysphagia include acute cerebral conditions, degenerative disorders, and trauma, disease, or surgery to the oro-pharyngo-oesophageal tract
Dysphagia has important implications in terms of management of patients, outcomes, and healthcare costs
Early and accurate evaluation and intervention are essential and the province of all clinicians
Box 1 : Common causes of dysphagia
Gastro-oesophageal reflux—waterbrash, regurgitation, due to dysmotility or stricture
Achalasia—classically hold-up relieved by carbonated beverages
Motility disorders—may be associated with central chest pain, systemic disease (scleroderma, dermatomyositis)
Oesophageal cancer—progressive, weight loss
Head and neck cancer—pain, dysphagia, otalgia, >90% smokers, often excess alcohol consumption
Pharyngeal pouch—slowly progressive, regurgitation, gurgling (fig 1)
Web—able to swallow only small amounts, “can't swallow tablets”
Stroke
Neurodegenerative disorders—parkinsonism, motor neurone disease, multiple sclerosis, myasthenia gravis
Presbyphagia
Sources and selection criteria
We used the search terms “swallow,” “dysphagia,” and “deglutition” to search PubMed, Medline, OVID, and CINAHL. We have incorporated the consensus from key texts and recent reviews with a range of foci.3–5 We all work closely together in the management of adult patients with swallowing disorders. We are experienced in flexible endoscopy of the upper airway, videofluoroscopy, manometry, and rehabilitation of the compromised swallow.
Incidence and causes
The incidence of squamous carcinoma of the oesophagus varies greatly from under 10 per 100 000 in developed countries to over 150 per 100 000 in Asia.6 Adenocarcinoma of the oesophagus is one of the fastest growing cancers in the Western world, constituting 34% of all oesophageal cancers and affecting mainly men (ratio 7:1).7 Barrett's oesophagus carries a hundredfold increased risk of adenocarcinoma.8
The demographic shift upwards in the age profile of the population results in increased numbers of people at risk of age related illness such as Parkinson's disease. Dysphagia complicates up to two thirds of cases of stroke and is linked to the reported incidence of chest infection in stroke.9 Healthy ageing affects the swallowing process (presbyphagia), and this may have serious consequences.10 Alternatively, changes with age may be misattributed to impaired swallowing. Over 50% of residents in long term care facilities have feeding difficulties, dysphagia, or both,11 and almost 30% of elderly people acutely admitted to hospital are dysphagic.12 Dysphagia also complicates multiple sclerosis, traumatic brain injury, and various psychiatric disorders.13–15 The causes and consequences of dysphagia are so diverse that patients are best managed where there is networked access to a range of different disciplines: gastroenterology, otolaryngology, speech and language therapy, nutrition, and neurology.
Normal swallow mechanism
The speed and complexity of human swallowing are essential because of the shared upper airway and foodway, which requires respiration to be suspended during the moment of swallow. Figure A on bmj.com shows the major structures and the location of events, and figure B shows bolus progression in more detail.

{kind=link}
Presentation and clinical features
Report by the patient is important and can often locate lesions accurately, but people have a tendency to identify the level of blockage at or above the site of the lesion.16 Thus cervical symptoms may originate at any point down to the gastro-oesophageal junction. Box 2 summarises the common and less obvious symptoms and the key findings at examination.
Box 2 : Symptoms of dysphagia and aspiration, and examination findings
Obvious symptoms
Difficulty swallowing
Heartburn
Coughing or choking before, during, or after swallowing
Globus
Regurgitation of “old” foodstuffs
Nasal regurgitation
Feeling of obstruction
Weight loss
Less obvious symptoms
Change in eating—for example, eating slowly or avoiding social occasions
Frequent throat clearing
Food avoidance
Prolonged meal times
Recurrent chest infections
Change in respiration pattern after swallowing
Atypical chest pain
“Wet” voice quality
Key examination findings
Angular stomatitis, glossitis (web)
Oral or oropharyngeal ulceration or swelling (head and neck cancer)
Neck mass (cervical lymphadenopathy, obstructive goitre)
Unexplained temperature spikes, wet or hoarse voice (aspiration)
Tongue fasciculation (motor neurone disease)
Vocal cord paralysis (cervical or thoracic neoplasia)
Aspiration of foreign material below the level of the true vocal cords (fig 2) may complicate dysphagia in as many as 75% of patients,17 with associated risks of pneumonia and death,18 especially in people with dysarthria.19 The most obvious sign that a person may have aspirated is the post-swallow cough, but other more insidious indicators may be present. Silent incidents with no clinical signs can account for over half of all cases of radiologically defined aspiration.20

Lateral fluoroscopic projection showing contrast material in the valleculas, pyriform sinuses, laryngeal vestibule, and aspiration into the upper trachea
{kind=link}
Globus sensation (feeling something “stuck” or “tightness” in the throat) may be confused with dysphagia. Patients are typically most aware of this during dry (saliva) swallows, and specific questioning of these patients reveals no true hold up of food passage and no need for dietary modification.21
Investigations
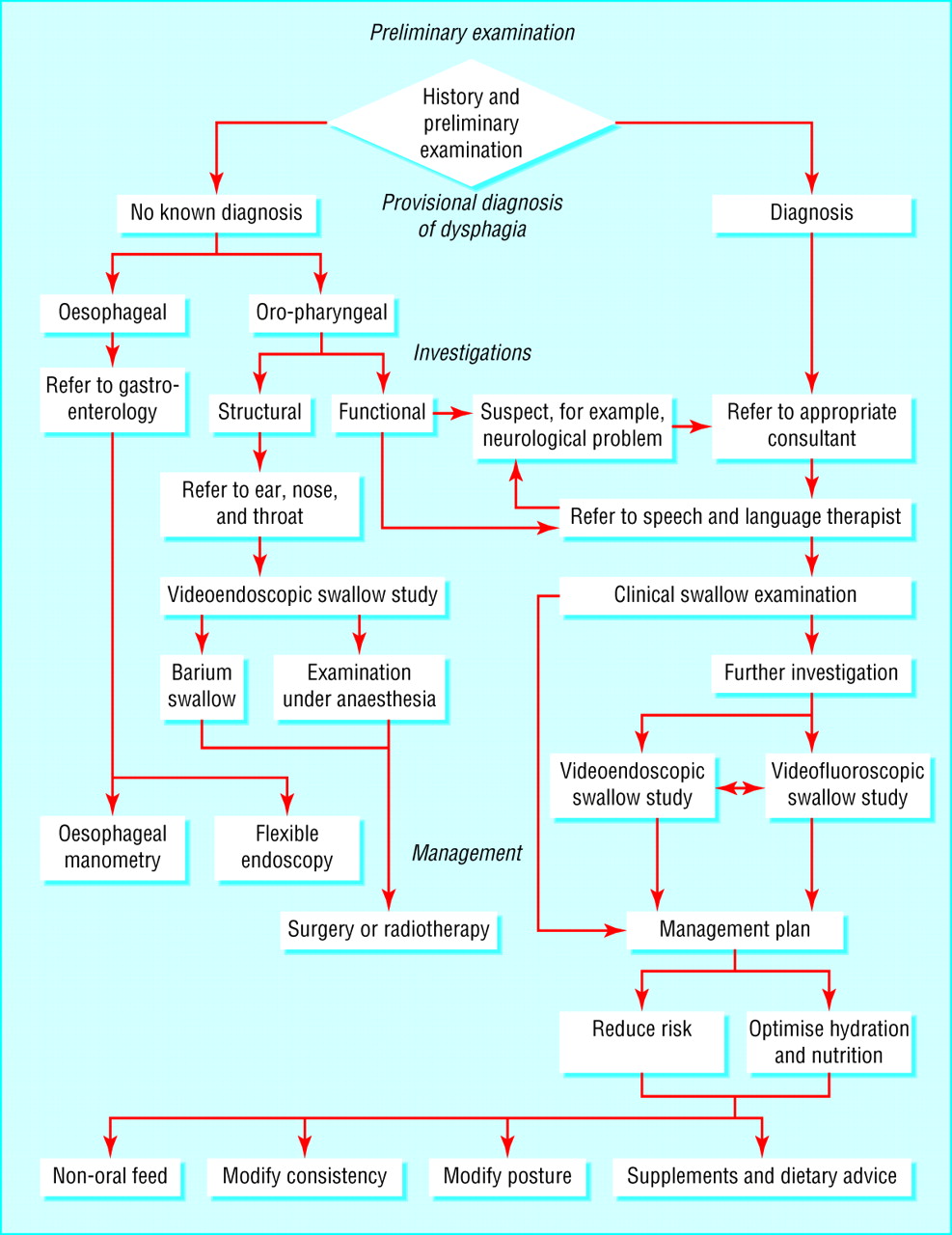
A careful case history and clinical examination may allow the clinician to identify the underlying pathology (right side of fig 3), in which case the patient is referred to the most appropriate speciality. Dysphagia of unknown aetiology clearly requires detailed investigation to establish the cause (left side of fig 3). Reported food obstruction below the clavicles requires primary investigation with either upper gastrointestinal endoscopy or barium swallow.

Flow chart for the investigation and management of dysphagia
{kind=link}
Endoscopy
Endoscopy has the advantage of potentially yielding a histological diagnosis. The overall rate of oesophageal perforation after flexible endoscopy involving oesophageal instrumentation, biopsy, or dilatation is 2.6%.22
Barium swallow
Barium swallow may be more readily available and will show cervical oesophageal lesions such as a web or pouch, but post-cricoid cancer may be missed. This procedure is contraindicated in suspected aspiration: instead of the desired “full column” barium delineation of the oesophagus, it may render a spectacular and hazardous bronchogram.
Oesophageal manometry
Oesophageal manometry remains the investigation of choice in suspected motility disorders.23 Manometry can classify oesophageal dysmotility into rare specific disorders such as achalasia and diffuse oesophageal spasm or more common non-specific motility disorders that do not respond directly to drug treatment but may improve if related reflux or psychiatric disturbances are treated.24 The symptoms of non-specific motility disorders may have an uncertain relation to the manometric abnormalities.25
Modern manometric strain gauge assemblies with computer recorders have very fast response times and are sensitive enough to capture the rapid sequence of events in the pharyngo-oesophageal segment. This has made possible ambulatory manometry, which is especially valuable for patients with intermittent symptoms such as chest pain.26 Ambulatory pH monitoring remains the gold standard when reflux is a possible cause of dysphagia.27 It is useful in patients with atypical symptoms or who have failed trials of antireflux treatment.28
Fibreoptic examination
Occasionally the referring clinician must choose the specialist by “best guess.” Is the disorder truly cervical (otolaryngological), or is it referred from the lower oesophagus (gastroenterological)? Patients with high dysphagia referred for ear, nose, and throat assessment will undergo clinical examination of the oral cavity and neck. The check for upper aerodigestive tract cancer is completed by fibreoptic examination of the hypopharynx and larynx. This may show the “rising tide” sign of pharyngeal diverticulum but will not identify post-cricoid cancer. If a vocal cord paralysis is present, this may indicate local tumour involvement or a mediastinal extension of, for example, an oesophageal tumour. Suspected laryngopharyngeal neoplasia is further assessed by examination under anaesthesia and staging computed tomography.
Clinical swallow assessment
Functional as opposed to structural oropharyngeal dysphagia requires a specific dynamic swallow assessment. This includes a formal clinical swallow assessment and, if appropriate, a videofluoroscopic or fibreoptic endoscopic evaluation of swallowing. In some cases the speech and language therapist may suspect a hitherto undiagnosed disorder and referral would be made to the appropriate specialist in conjunction with the swallow assessment.
Clinical swallow assessment by a specialist speech and language therapist is the most appropriate way to fully assess the nature and impact of oropharyngeal dysphagia and screen for risk of aspiration.29 The main components are (a) detailed case history of factors affecting the swallow process; (b) assessment of general mental and physical status; (c) oromotor examination, including specific motor power and range; and (d) observation of the patient swallowing boluses controlled for size and consistency.30 Oropharyngeal sensation evaluated by a detailed examination is a sensitive predictor of swallow competence31; simply noting the presence or absence of the gag reflex is not.
A typical assessment starts with teaspoonfuls of water, and observations include oral phase bolus preparation; timing of swallow (triggers with no delay); laryngeal elevation and coordinated movement; and signs of aspiration before, during, or after swallowing (box 2). If appropriate, 100 ml of water is offered to assess continuous swallowing and the same observations are made together with the rate and total volume managed.32 Difficulties with any of these stages indicate a risk of aspiration. More challenging boluses are investigated in the same way if appropriate.
Videofluoroscopic swallow study
Videofluoroscopic swallow study or “videofluoroscopy” is ideally performed by a consultant radiologist and specialist speech and language therapist.33 The real time video radiographic image provides visualisation of the structures, movement, and coordination of swallowing. Abnormal oropharyngeal and oesophageal anatomy can be readily identified. Videofluoroscopy allows an in-depth examination of the cause of aspiration and what remedial action, such as modification of posture or food consistency, will help.34 As with the clinical swallow assessment, a range of bolus types and sizes must be systematically investigated. Access to videofluoroscopy varies, and where it is scarce priority should be given to complex cases in which the clinical swallow assessment is not adequate to manage the patient “at bedside.” Increasing evidence shows that radiologically defined aspiration does not necessarily indicate clinical complications or potentially poor long term outcome,35 and it should be used to see why and not just if a person aspirates.
Fibreoptic endoscopy
Fibreoptic endoscopic evaluation of swallowing by a specialist speech and language therapist involves passing a flexible endoscope through the nasal cavity to visually assess the function of the larynx and pharynx (fig C on bmj.com).30 The key abnormalities best detected by endoscopic evaluation are of palatal function, vocal fold mobility and closure, degree and location of post-swallow residue, and pharyngeal and laryngeal sensation.36 Pre-swallow and post-swallow aspiration can be accurately identified by endoscopic swallow studies,37 whereas aspiration at the moment of swallow is best observed by videofluoroscopy.36 Endoscopy, unlike videofluoroscopy, can be used for multiple or serial examinations and patient biofeedback.
Formulating a management plan
Management is based on the history, findings of the clinical investigations, and prognosis for the individual patient (fig 3). The underlying disorder is treated, but the impact of dysphagia on nutrition and hydration will compromise any intervention unless managed effectively. Poor physical condition from malnutrition or dehydration will lead to a suboptimal rehabilitation process, in both duration and completeness of recovery,38 and inadequate management of dysphagia contributes to this. A malnourished person is at risk of decompensation of the swallow, leading to dysphagia.39 The clinical swallow assessment is used to determine safe modified diets that reduce malnutrition and dehydration. This may range from nil by mouth with total enteral support to full oral route or a balance of the two. Enteral feeding is essential to maintain nutritional status when oral feeding is suspended, even if only for a short time.40 Prompt involvement of a dietitian is thus essential.
A multidisciplinary network is essential in managing patients with dysphagia. Timely intervention can prevent or ameliorate the complications of dysphagia. The supervising clinician, whether in general practice or an acute hospital specialty, can contribute to this by following the guidelines set out here. This should result in fewer patients having dysphagia, and for a shorter duration, thus optimising patient care and reducing the burden for all healthcare providers.
Footnotes
-
Competing interests None declared.
-
 Three additional figures are on bmj.com
Three additional figures are on bmj.com