Article Text

Abstract
Background: The transradial approach for percutaneous coronary procedures has the advantage of reduced access site complications but is associated with specific technical challenges in comparison with the transfemoral approach. Transradial procedure failures can sometimes be due to variation in radial artery anatomy. However, data describing such variations are limited.
Objective: To evaluate the incidence and impact of radial artery anomalies in patients undergoing transradial coronary procedures.
Methods: Retrograde radial arteriography was performed in all patients presenting for a first-time radial procedure. Patient characteristics, radial artery anatomy and procedural outcome were assessed.
Results: 1540 consecutive patients were studied, 70.6% male, mean (SD) age 63.6 (11.1) years. The overall incidence of radial artery anomaly was 13.8% (n = 212). 108 (7.0%) patients had a high-bifurcating radial origin, 35 (2.3%) had a full radial loop, 30 (2.0%) had extreme radial artery tortuosity and 39 (2.5%) had miscellaneous anomalies such as radial atherosclerosis and accessory branches. Overall transradial procedural success was 96.8%. Procedural failure was more common in patients with anomalous anatomy than in patients with normal anatomy (14.2% vs 0.9%, p<0.001). Procedural failure in patients with high radial bifurcation, radial loop, severe radial tortuosity and other anomalies was 4.6%, 37.1%, 23.3% and 12.9%, respectively. 15 (1%) vascular complications occurred, all of which were treated conservatively without ischaemic sequelae.
Conclusion: Anomalous radial artery anatomy is relatively common and is a significant cause of procedural failure. Within each specific anomalous pattern there is a differential procedural failure rate. This has implications for clinical practice and suggests a need for imaging of the radial artery after sheath insertion.
Statistics from Altmetric.com
Since its initial description as a safe and feasible access route for cardiac catheterisation1 2 the radial artery has increasingly been used for percutaneous coronary procedures. The main advantage over the femoral artery is a reduced risk of vascular complications, particularly in the presence of multiple antiplatelet and antithrombotic agents.3–9 This is attributed to the favourable neurovascular anatomy of the radial artery where it runs superficially, separated from major nerves. Immediate ambulation and facilitation of day-case intervention also favour the radial approach.10–13 The transradial technique is, however, associated with a significant learning curve even for experienced femoral operators.14–17 Although procedure failures may sometimes be due to radial artery anatomical variations, there are limited data describing such variations.18 We undertook to establish the frequency of radial artery anomalies and their relation to procedure outcome in patients undergoing a first transradial coronary procedure.
MATERIALS AND METHODS
Study population
This was a multicentre prospective study involving four tertiary centres in the UK. A total of 1540 consecutive patients undergoing their first transradial coronary procedure were recruited from January 2006 to June 2007. Only patients undergoing diagnostic angiography and coronary intervention were studied. Procedures were performed or supervised by experienced high-volume radial operators (trainers with a personal experience of >1000 cases, trainees >100 cases). Patients with a previous transradial procedure were excluded.
Radial artery cannulation
Radial artery puncture was performed with a dedicated radial cannulation needle and guidewire according to operator preference. A short hydrophilic sheath (11 cm) was inserted and an arterial vasodilator (containing 200–400 μg isosorbide dinitrate and 2.5–5.0 mg verapamil) given according to local protocols. Heparin (2500–5000 IU) was given either as part of the vasodilator cocktail or in the aortic root.
Retrograde radial arteriography
Retrograde radial arteriography was performed after administration of the arterial vasodilator to define radial artery anatomy from mid-radius to radiobrachial anastomosis. A solution of 3 ml of contrast mixed with 7 ml of blood (to dilute the contrast and minimise any discomfort from contrast injection) was injected briskly through the side arm of the sheath with radiographic acquisition at the elbow in an anteroposterior projection. If a high-bifurcating radial origin was identified, a further arteriogram was obtained higher up the arm to identify the point of anastomosis to the brachial artery.
Transradial coronary procedures
Retrograde radial arteriography was performed before coronary intubation in all patients. In patients who had a failed transradial puncture, it was at the discretion of the operator to attempt the contralateral radial artery or use the transfemoral approach. The arterial sheath was removed immediately after completion of the transradial procedure and haemostasis achieved using a unilateral radial compression system (RADI-Stop; RADI Medical Systems, Uppsala, Sweden or TR Band; Terumo Medical, Tokyo, Japan).
Classifications and definitions
Forearm arterial patterns with clinical relevance to transradial cardiac catheterisation were classified using a modification of McCormack’s, Uglietta’s and Rodriguez-Niedenfuhr’s definitions.19–21
The site of anomalous origin was determined with reference to the intercondylar line of the humerus, which is a fixed line representing the proximal border of the antecubital fossa. Bifurcation of the brachial artery proximal to this line is considered a variant pattern. A high-bifurcating origin was further subclassified into lower third of humerus, middle third of humerus, upper third of humerus or axillary according to the site of anastomosis with the main vessel. High-bifurcating radial artery calibre was also categorised as <2.0 mm, 2.0–<2.5 mm, 2.5–3.0 mm and >3.0 mm by visual comparison with the arterial sheath.
A radial artery loop was defined as the presence of a full 360° loop of the radial artery distal to the bifurcation of the brachial artery. Extreme radial tortuosity was defined as the presence of a bend of more than 90° in the contour of the vessel. Anatomical variations that did not fit into these specified categories were grouped together and categorised as “other” anomalies.
Procedural duration was defined as the time interval between when the patient entered to when they left the catheterisation laboratory. Procedural success was defined as completion of the planned procedure through the initially selected radial access route. Minor vascular complications were defined as haematoma <5 cm, vessel dissection without ensuing ischaemia, pseudoaneurysm and localised infection. Major vascular complications were defined as haematoma >5 cm, any access site complications that required surgical or radiological intervention, >30 g/l haemoglobin drop due to access site bleeding, bleeding requiring transfusion, limb ischaemia and/or compartment syndrome.
Data collection
Patient demographics, procedural data and radial arteriography findings with specific details of any anomalies and local vascular complications were collected on a specifically written data management database (PATS Dendrite).
Statistical analysis
Statistical analysis was performed using SPSS 14.0 for Windows. Categorical data were presented as absolute values and percentages, whereas continuous data were presented as mean (SD). The nature of distribution of the data was determined using a one-sample Kolmogorov–Smirnov test. A Student t test and Mann–Whitney U test were used to compare continuous data, as appropriate. Categorical data were compared using the χ2 test with the appropriate degree of freedom. Both univariate and multivariate regression analysis were used to examine potential correlation between radial artery anomaly and variables such as sex, age, hypertension, diabetes and peripheral vascular disease. A p value <0.05 was considered to be significant.
RESULTS
Patients and procedural characteristics
A total of 1540 patients were studied with mean (SD) age 63.6 (11.1) years and 70.6% male. Table 1 summarises baseline patient and procedural data. Diagnostic coronary angiography was performed in 32.8%. Most procedures were attempted via the right radial artery and over 50% of procedures were performed using 5F sheaths and catheters. Transradial procedural success was 96.8% with 2.9% of patients requiring femoral access for procedure completion. Procedures were abandoned in 0.3%.
Radial artery anatomy and procedural outcome
Seven cases (0.5%) of radial puncture failure occurred. Retrograde radial arteriography was obtained in 1533 patients. Anomalies were noted in 212 (13.8%) and these patients were significantly older (mean age 67.1 vs 64 years, p<0.001) more commonly female (36% vs 28%, p = 0.02) with significantly higher procedure failure rates (14.2% vs 0.9%, p<0.001) (fig 1). Although procedure duration and fluoroscopy time were longer in patients with anomalies, these were not statistically significant.

Normal radial artery anatomy
Normal radial artery anatomy (fig 2) was present in 1321 patients (86.2%). Transradial failure rate was low in patients with normal radial anatomy, with 12 failures out of 1321 patients (0.9%). Procedure failures were due to profound radial artery spasm (five patients, 0.4%), severe brachial artery stenosis (one patient, <0.1%), tortuous subclavian artery (four patients, 0.3%), radial artery dissection (one patient, <0.1%) and dissection of axillary artery (one patient, <0.1%).

Radial anomalies
Figure 3 summarises the anomaly types and associated failure rates. Table 2 compares patient characteristics and procedural data for different radial anatomical patterns. Patients with radial artery loops were significantly older than patients with normal anatomy or high bifurcation while extreme radial tortuosity was seen in the oldest group. Age was the only independent predictor related to the presence of radial artery anomaly.

High-bifurcating radial origin
This was the most common radial anomaly (fig 4) seen in 108 patients with an incidence of 7.0%. The majority of these vessels rejoined the brachial artery at the level of mid- or upper humerus and were of small calibre with over 85% being <3 mm in diameter (fig 5). Importantly, although a high-bifurcating radial artery was not associated with a high incidence of transradial failure (5/108 patients; 4.6%), many of these anomalous vessels were of small calibre and frequently required the use of 5F catheters with hydrophilic wires to complete the procedure without inducing spasm.


Radial artery loop
A radial artery loop was seen in 35 patients (2.3%). These mostly involved the proximal radial artery just below the brachial bifurcation. A recurrent radial artery (occasionally two) was noted to arise from the apex of the loop in all cases, which was of small calibre and invariably assumed a straight path into the upper arm. The presence of a radial loop was associated with a high procedural failure rate with 13 out of the 35 procedures (37.1%, p<0.001) failing to complete. Seven of thirteen patients had unfavourable radial loop anatomy with large diameter loops (fig 6). These were considered to be insurmountable by the experienced radial operators and the procedure was abandoned from this access site. In the remaining 22 patients, the radial loops had a smaller diameter and were “crossed” with a hydrophilic or an angioplasty wire. With the loop straightened, the procedure was successfully completed (figs 7A and B).


Extreme radial artery tortuosity
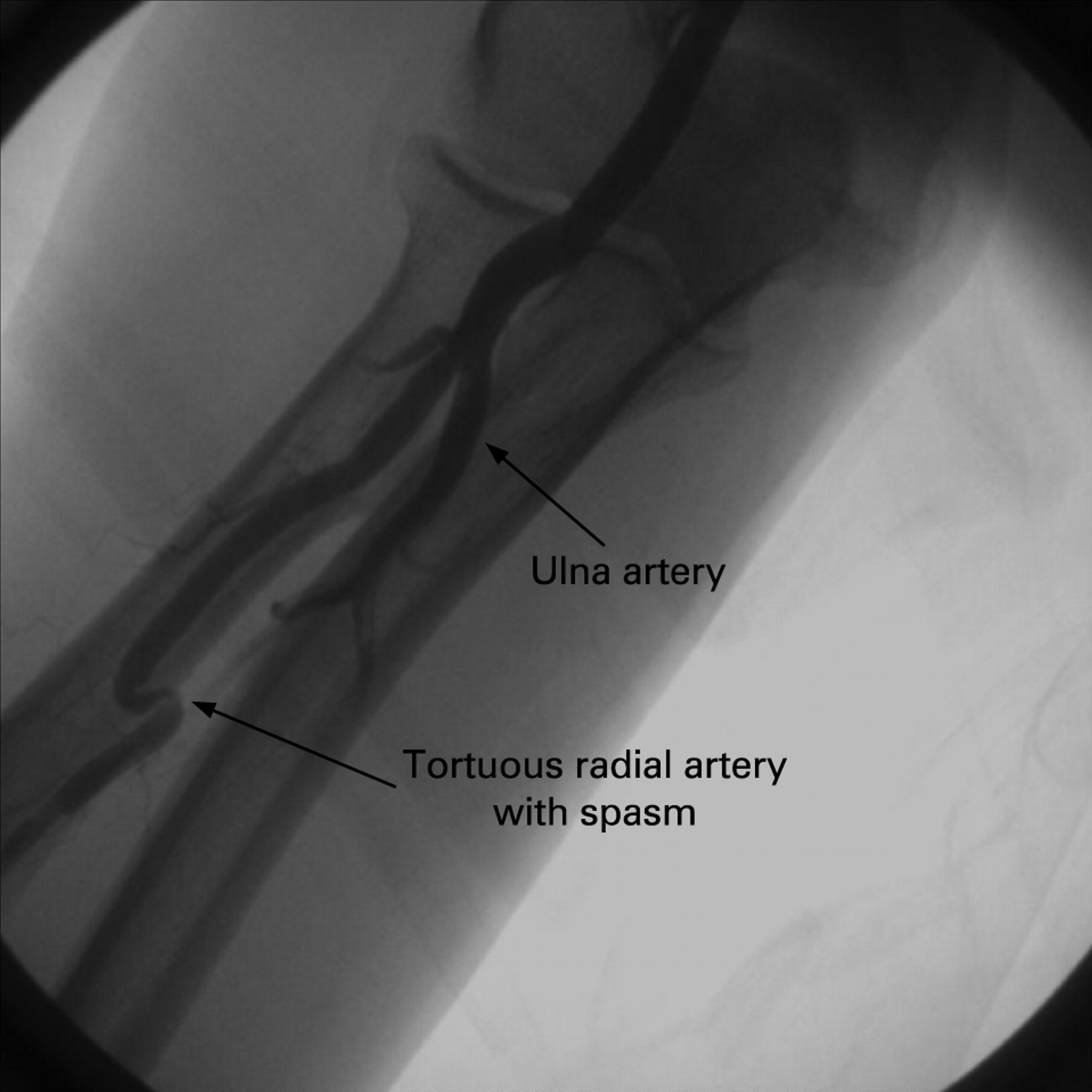
Extreme radial artery tortuosity (fig 8) was seen in 30 patients (2.0%). The presence of extreme radial tortuosity was also associated with a high procedural failure rate with seven failures (23.3% p<0.001). These vessels were prone to severe radial artery spasm; this being the reason for procedure failure in all cases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Other anomalies
Various other anomalies were present in 39 patients, giving a combined incidence of 2.5%. In 17 patients there was evidence of radial atherosclerosis (1.1%). Of clinical interest, in all such patients it was possible to cross with guidewires and catheters. However, in five patients (29.4%) there was procedural failure due to extreme subclavian tortuosity. In the remaining 22 patients a range of minor anatomical variations (such as anomalous additional vessels and minor bifurcation variations) were present. These had no clinical significance since all cases were completed via the chosen radial access site.
Vascular complications
No patients had bleeding requiring transfusion or surgical intervention. Access site vascular complications in 15 patients (1.0%) were treated conservatively. These were: small haematoma (eight), large haematoma (two), radial artery dissection (two), immediate radial artery occlusion (two) and axillary artery dissection (one). Two patients with large haematoma were successfully treated with customised compression and arm elevation without evidence of compartment syndrome or hand ischaemia. The patient with axillary artery dissection was also managed conservatively without ischaemic sequelae.
DISCUSSION
Transradial percutaneous coronary procedures have gained in popularity because of reduced access site vascular complications and immediate patient mobilisation. Procedural success has been facilitated through technological enhancements and miniaturisation of equipment. Reported technical failure for transradial procedures is between 1% and 5%,3 22–24 compatible with our overall figure of 3.2%. There are several reasons leading to failure: inability to puncture, artery spasm and anatomical variations. Whereas incidence of the first two of these causes is documented,3 22–24 information relating to radial artery anatomical variation is limited. Furthermore, there is a paucity of data on the presence of radial artery anomaly and its relation to procedure failure. Our data define radial artery anomalies in patients undergoing a first transradial cardiac procedure. Furthermore, we observed higher procedure failure rates in patients with radial artery anomaly, and of clinical interest, different anomalies were associated with different failure rates even for experienced operators.
Autopsy studies of upper limb arterial anatomical variation reported a frequency of between 4% and 18.5%.19 21 25 When two-dimensional ultrasonography and colour Doppler were used this figure was 9.6%,26 while arteriography studies reported between 7.4% and 22.8%.20 27 28 Not only were there wide variations in the occurrence of anomaly but there were also variations in the pattern of anomalies reported, partly owing to differences in definitions. The incidence of anatomical variation was higher in autopsy studies as variation was defined according to the course of the artery in relation to muscle and nerve that would not be evident in arteriographic studies.
An interesting observation from the autopsy studies was an absence of radial artery tortuosity or hypoplasia. One explanation is that radial artery tortuosity is only seen in the presence of a dynamic arterial circulation and therefore not seen at autopsy. The absence of hypoplasia in autopsy studies might be explained by arteriographic studies reporting existence of “normal” arteries with severe spasm.28 Radial artery hypoplasia was not reported in our study nor that by Yoo et al,27 and Louvard and Lefevre.18 It is also worth noting that radial artery loop was not a separate category but under the category of variation of anastomosis between brachial artery and radial or ulnar artery at elbow level. Furthermore, not all such anastomosis variations were full 360° loops as variations could be either in the form of a sling-like loop or rectilinear pattern.29 There is therefore no reported frequency of isolated full 360° radial loop from autopsy studies.
The most common radial artery anomaly seen is high radial bifurcation, with a reported frequency range of 0–14.3%. The absence of high radial bifurcation was reported using ultrasonographic scanning, suggesting that it is not reliable in identifying this type of anomaly.26 However, the small sample size and racial variation (115 exclusively Japanese patients) may have been contributory. Yoo et al reported a radial bifurcation incidence of 2.4% in 1191 Korean patients.27 The reported 7.0% in our study was comparable to the 8.3% reported by Valsecchi et al28 but lower than the 14% in autopsy studies.19 21 Importantly, our study confirmed that this anomaly did not significantly impact on procedural success. In patients with high radial bifurcations with small calibre proximal artery, the use of 5F equipment and/or a hydrophilic wire was required for procedure completion.
The presence of a radial artery loop is the commonest cause of procedure failure for experienced radial operators.18 The 2.3% frequency of a full 360° radial artery loop in our study is the highest reported. All loops were accompanied by a recurrent radial artery at the apex of the loop which invariably assumed a straight path into the upper arm. The presence of the remnant recurrent radial artery has potential to complicate the crossing and straightening manoeuvre, with a tendency for the wire to selectively “follow” the path of the remnant artery, thereby increasing risk of dissection or perforation especially if such anatomy has not been initially defined.
Although loops can often be crossed using either a hydrophilic or an angioplasty wire and then straightened with a 5F JR4 configuration diagnostic catheter, these manoeuvres can induce spasm and pain, making subsequent catheter manipulation and advancement impossible. Our procedure failure rate of 37.1% in patients with a radial loop was high. However, more than half of these were patients with large-diameter radial loop anatomy deemed impassable after radial arteriography, and procedures were completed via alternative access sites without attempting to cross the loops. The early definition of such anatomy at procedure outset informed the operator, thereby avoiding potential complications.
Extreme radial artery tortuosity was also associated with significant procedure failure (23.3%). Our strict definition for extreme tortuosity differed from other studies with a consequent lower incidence of 2.0%, compared with 3.8%, 4.2% and 5.2% by Valsecchi et al, Yoo et al and Yokoyama et al, respectively.26–28
Other anomalies seen in our study included a low incidence of radial atherosclerosis. This may be an important marker for extensive extracardiac vascular disease as many such patients were found to have tortuous subclavian vessels that could not be navigated, leading to procedural failure. Other minor variations in bifurcation anatomy had no influence on procedural outcome.
The acquisition of a radial arteriogram requires only a minimal contrast load, a small amount of additional radiation and trivial extra procedural time. This is offset by the provision of important information that aids the operator in planning an optimal procedure.
CONCLUSION
Radial artery anomalies are relatively common and a cause of transradial procedure failure even for experienced radial operators. Retrograde radial arteriography helps to delineate underlying anomalies, identifying patients with unfavourable anatomy and thereby helping the operator to plan a strategy to overcome the anomaly or change access route with the potential to save time and avoid vascular complications. This can be performed with a minimum of contrast (3 ml) and should be considered part of a routine transradial procedure.
REFERENCES
Footnotes
-
Competing interests: None.