Article Text

Abstract
OBJECTIVE To compare the coronary anatomy and the location of coronary lesions in monozygotic and dizygotic twin pairs affected with coronary artery disease.
DESIGN Coronary angiographic findings were compared with respect to the distribution of coronary blood supply and the location of coronary lesions.
MAIN OUTCOME MEASURES Distribution of coronary blood supply, diameters and length of proximal coronary arteries.
RESULTS The lumen diameters of the left main coronary artery, the left anterior descending coronary artery, the circumflex artery, and the right coronary artery, as well as the lengths of the left main coronary artery, showed similar variability within monozygotic and dizygotic twin pairs. With respect to the dominance pattern of coronary blood supply, two of three monozygotic twin pairs differed, while all dizygotic twin pairs were concordant. Concordant and discordant locations of stenoses were found with similar frequency in monozygotic and dizygotic twin pairs.
CONCLUSIONS The dominance pattern of coronary blood supply and the location of coronary lesions are not strictly hereditary. The high concordance of premature coronary artery disease found in monozygotic twin pairs may largely be related to factors that are independent of the macroanatomic distribution of the coronary blood supply.
- twin studies
- coronary anatomy
- coronary lesions
Statistics from Altmetric.com
Monozygotic twins have been shown to have a high concordance for coronary artery disease.1 The chance of dying from coronary heart disease within 10 years is almost 50% for a 55 year old man if his monozygotic twin had a fatal myocardial infarction.1 This risk is about 20 times higher than for a representative individual in the overall population and 3.2- to sixfold higher than for the dizygotic twin of a patient with myocardial infarction.1 The question arises as to what mechanisms account for such a high concordance for myocardial infarction in the second monozygotic twin. We speculated that as well as having inherited risk factors affected monozygotic twins may share the anatomy of their coronary arteries. In this respect it has been well documented that certain anatomical features may precipitate coronary atherosclerosis and occlusion.2 However, it is unknown whether the coronary anatomy in monozygotic twins is identical, as few case reports have evaluated this.3-7 In order to study the heredity of coronary anatomy in more detail we compared the coronary arteries in three monozygotic and three dizygotic twin pairs by measuring key anatomical features and the location of coronary lesions.
Methods
Three monozygotic and three dizygotic twin pairs were identified retrospectively by screening of 93 500 patient records in seven cardiac rehabilitation centres. All individuals had symptomatic premature coronary heart disease and were thus studied by cardiac catheterisation. All participants gave written informed consent for study of genetic risk factors for myocardial infarction.
Anthropometric data, risk factors, and clinical events were taken from the patients' records. Obesity, hypertension, and dyslipidaemia were defined as previously suggested.8 To document monozygosity and dizygosity, all participants were genotyped with respect to the allele status of six biallelic polymorphisms and two polymorphic markers.
ANALYSIS OF CORONARY ANATOMY
Coronary blood supply was defined according to Baim and Grossmann.9 The prevalence of right dominant, left dominant, and balanced circulation is 85%, 8%, and 7%.9
The proximal luminal reference diameters of the left main coronary artery, the left anterior descending coronary artery, the circumflex artery, and the right coronary artery were measured with calipers after threefold enlargement by projection on a screen. Measurements of the diameters of the contrast filled coronary catheters allowed us to extrapolate the absolute luminal coronary diameters. The length of the left main coronary artery was extrapolated in the same way. Quotients of vessel diameters were also determined as follows: right coronary/left main, left anterior descending/left main, circumflex/left main, and circumflex/left anterior descending.
The location of stenoses was attributed to coronary segments10 and the percentage of the stenoses was measured as minimum lumen diameter divided by reference diameter × 100. A coronary lesion compromising the lumen by more than 50% was considered to represent a stenosis.
Results
Clinical features are shown in table 1. Genotyping revealed complete concordance in all monozygotic twin pairs. In contrast, discordance of at least one of the polymorphic markers was evident in all dizygotic twin pairs.
Risk factors and anthropometric and clinical characteristics
CORONARY ANGIOGRAPHY
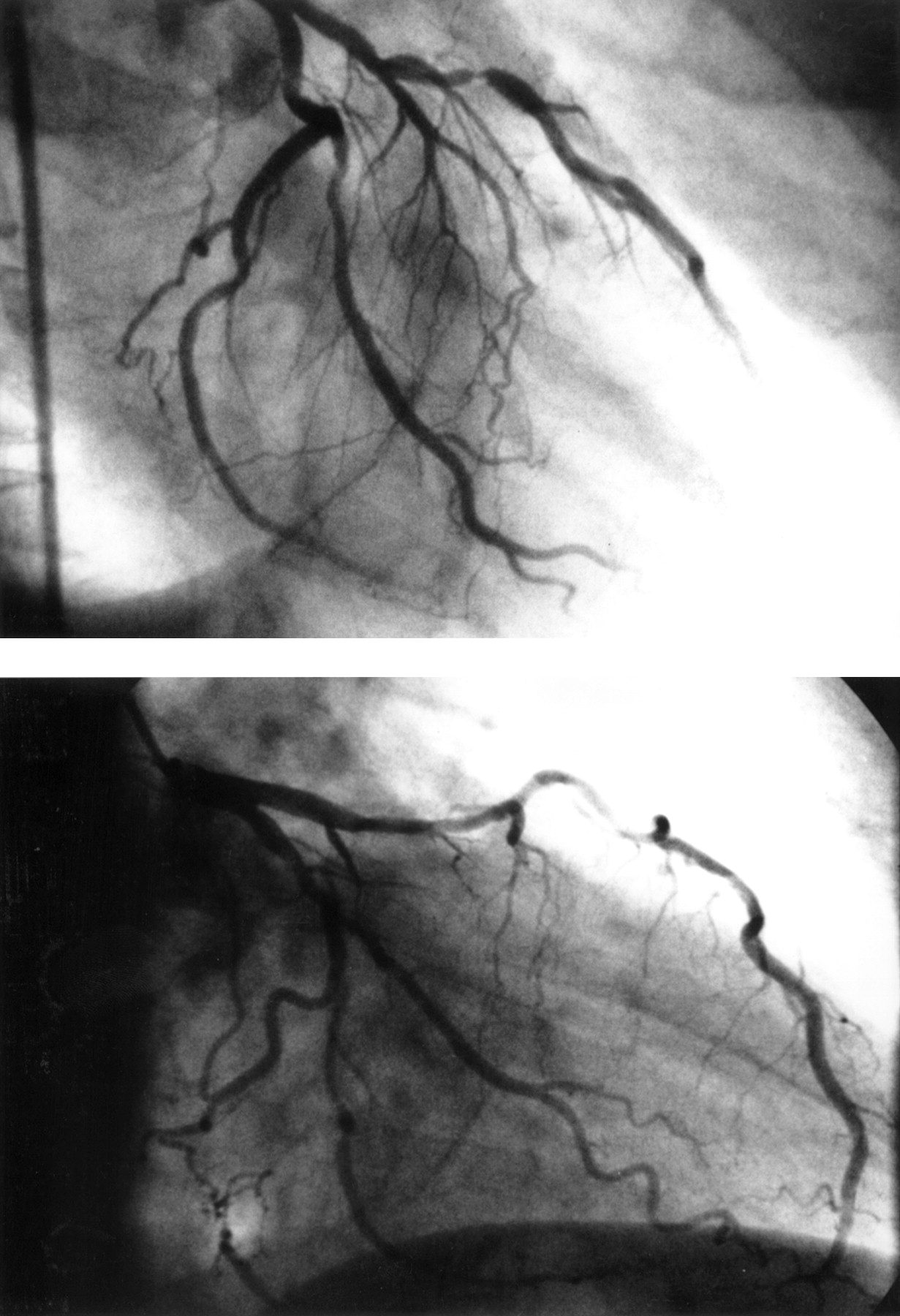
Figure 1 shows the right coronary arteries of twin pair No 3, both being occluded in the proximal segment of the vessel. The periphery of the artery in the lower panel is filled by right to right collaterals. While the appearance of the arteries in fig 1 is rather similar, differences were observed in the monozygotic twin pair No 2 (fig 2). The right coronary artery in fig 2 (left panel) is rather hypoplastic with a small posterior descending artery (balanced circulation). In contrast the right coronary artery in fig 2 (right panel) of the respective monozygotic twin sister is large and by definition dominant. The left coronary arteries in fig 3 appear to have a high concordance. Of the monozygotic twin pairs only a single pair showed concordance with respect to a balanced circulation, while two were by definition discordant. All dizygotic twin pairs were concordant for the rather frequent right dominant circulation.
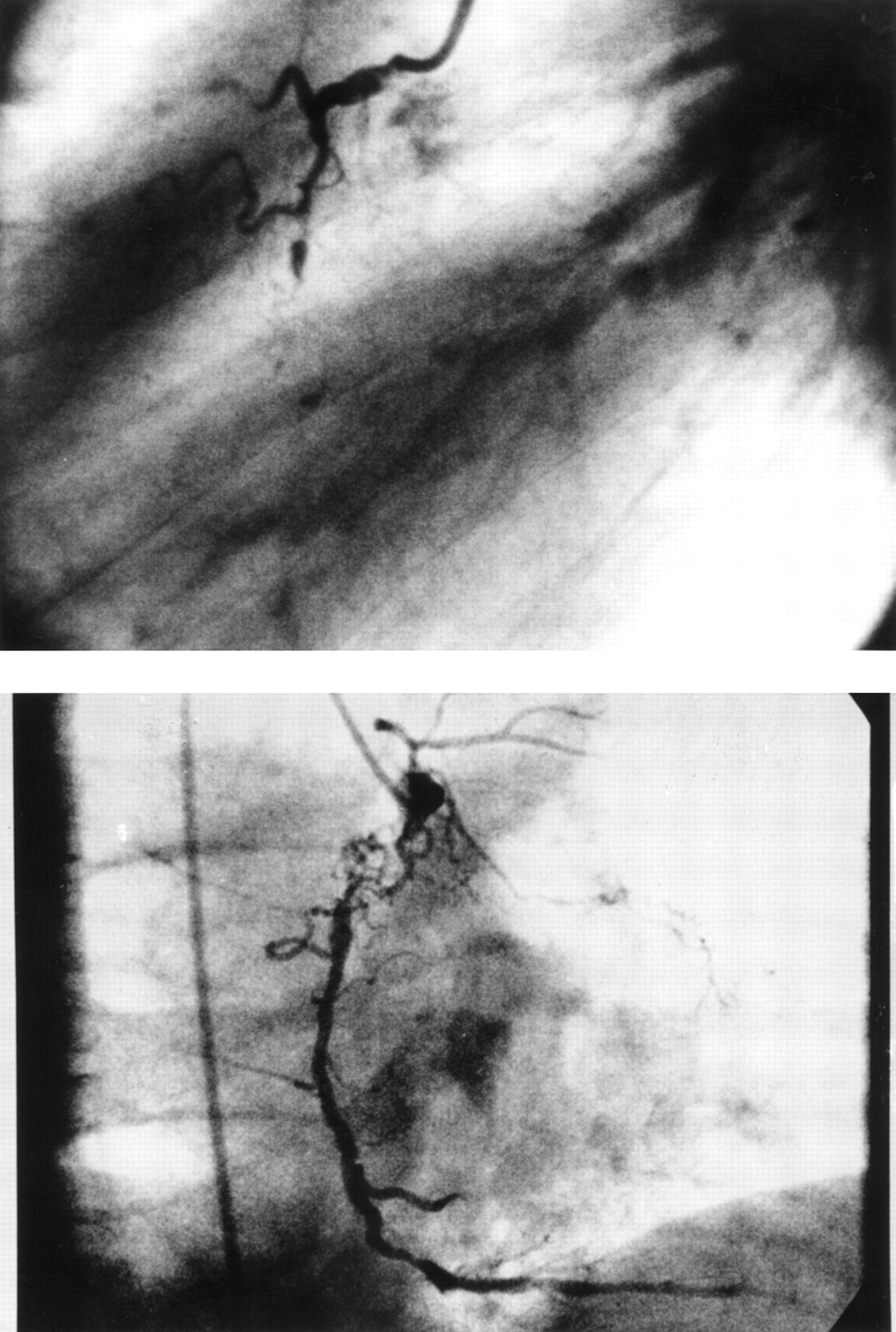
Right coronary arteries of twin pair 3. Both arteries are occluded in the proximal segment. The periphery of the artery in the right panel is filled by right to right collaterals.

Right coronary arteries of twin pair 2. The artery in the left panel shows a balanced circulation while the artery in the right panel shows a right dominant circulation.

Left coronary arteries of twin pair 3. The marginal branches in particular show very similar proportions.
MEASUREMENTS OF THE CORONARY DIAMETERS
Diameters and lengths of the coronary arteries are shown in table2. There was no obvious concordance in monozygotic twin pairs. We also calculated the relative size of the vessels with reference to the left main coronary artery. Comparing these ratios, we saw a slightly smaller difference in the variability between monozygotic compared with dizygotic twins (fig 4), but these differences did not reach statistical significance. Likewise, there was no obvious concordance in the lengths of the left main arteries in monozygotic twins.
Diameters and length of coronary arteries

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean differences of the relative lumen diameters of defined coronary arteries, expressed as quotients, within monozygotic and dizygotic twin pairs. White bars represent monozygotic twins, black bars represent dizygotic twins. Error bars = SEM. CX, circumflex artery; LAD, left anterior descending coronary artery; L main, left main coronary artery; RCA, right coronary artery.
LOCATION AND PERCENTAGES OF THE CORONARY LESIONS
The location and the percentages of coronary lesions are shown in table 3. Altogether, we observed 17 lesions resulting in more than 50% stenosis in monozygotic twins and 11 such lesions in dizygotic twins. Lesions were found in the same coronary segment three times in both monozygotic and dizygotic twin pairs. With regard to all lesions observed, the rate of concordance was 35% in monozygotic twins and 54% in dizygotic twins.
Location of the stenoses
Discussion
Studying the angiographic coronary anatomy in three monozygotic and three dizygotic twin pairs, we obtained no evidence in support of the hypothesis that the coronary blood supply is strictly determined by hereditary factors. First, in this small series we observed differences in the right versus left dominance pattern of the coronary arteries more often in monozygotic twin pairs. Moreover, the variability in the relative size of the proximal coronary arteries varied considerably in monozygotic twins and was not substantially smaller than in dizygotic twins. Second, the location of the stenoses did not show a higher concordance in monozygotic than in dizygotic twin pairs.
In the past only a few case reports have described angiographic findings of monozygotic twin pairs with coronary heart disease.3-7 Some of these found a concordant coronary blood supply,3-5 while some did not.4 ,6 ,7While our study can provide examples of both concordant and discordant blood supply in monozygotic twins, it is the first to attempt a more systematic approach to analysing the heredity of the coronary macroanatomy by comparing monozygotic and dizygotic twin pairs. In addition, the present participants were genotyped for clear documentation of their respective zygosity. The findings show a similar variability in the coronary anatomy and the pattern of blood supply in groups of monozygotic and dizygotic twin pairs. Thus it appears that the pattern of coronary blood supply is not predominantly affected by shared genes but rather by local factors acting during cardiac development.11
All case reports except one7 have described similar locations of the coronary lesions in monozygotic twin pairs. In the present study, we compared the location of the stenoses in monozygotic twin pairs with those in dizygotic pairs and cannot confirm a strict heredity of the location of coronary lesions. There was, however, a high concordance of traditional risk factors in monozygotic twin pairs, suggesting that similar mechanisms might have been involved in the development of coronary heart disease.
The present series is limited by its small size, such that a formal statistical analysis had only moderate power to detect differences between the two groups. A further limitation is that coronary angiography was not carried out under highly standardised conditions. However, the obvious differences in coronary anatomy between monozygotic twins reported by previous investigators4 ,6 ,7 and in this paper make it unlikely that the coronary blood supply is strictly determined by genetic disposition.
We therefore conclude that the dominance pattern of the coronary blood supply or the location of coronary lesions are not identical in “identical twins” with coronary artery disease. Future studies with larger numbers of twin pairs may be needed to detect potentially smaller genetic effects on these two phenotypes or to confirm the predominance of non-genetic factors by means of a formal statistical analysis.
Acknowledgments
We wish to thank the University Hospital of Münster, the Marienhospital Osnabrück, the St Bonifatius-Hospital Lingen, and the Städtisches Klinikum Augsburg for performing the coronary angiography. Supported by the Deutsche Forschungsgemeinschaft (DFG Schu 672/9-1, 672/10-1, and 672/12-1), the Bundesministerium für Forschung und Technologie, and the Vaillant Stiftung.