Article Text

Abstract
Acute pancreatitis (AP) is characterised by inflammation of the exocrine pancreas and is associated with acinar cell injury and both a local and systemic inflammatory response. AP may range in severity from self-limiting, characterised by mild pancreatic oedema, to severe systemic inflammation with pancreatic necrosis, organ failure and death. Several international guidelines have been developed including those from the joint International Association of Pancreatology and American Pancreatic Association, American College of Gastroenterology and British Society of Gastroenterology. Here we discuss current diagnostic and management challenges and address the common dilemmas in AP.
- acute pancreatitis
Statistics from Altmetric.com
Epidemiology
The UK incidence of acute pancreatitis (AP) is estimated as 15–42 cases per 100 000 per year and is rising by 2.7% each year.1 AP has a mortality rate of 1%–7% which increases to around 20% in patients with pancreatic necrosis.2 The mortality rate is influenced by the severity of the disease with several prognostic factors having been described. The presence of persistent organ failure is associated with the highest mortality, which is as high as 60% in some series.3 Gallstone pancreatitis is more common in women over the age of 60, especially among those with microlithiasis, while alcoholic pancreatitis is more frequent in males.4
Aetiology
Several aetiological factors have been described for AP although in up to 30% of cases an aetiological factor cannot be identified (termed idiopathic pancreatitis).5 The presence of microlithiasis accounts for 80% of idiopathic pancreatitis.6 In the UK, gallstones followed by alcohol intake are responsible for 75% of cases of AP.5 The most common cause worldwide is alcohol consumption. Table 1 demonstrates other aetiologies.
Aetiology and pathogenesis of acute pancreatitis
Pathophysiology
The initiating event in AP is due to acinar cell injury and impaired secretion of zymogen granules and involves extracellular neural and vascular mechanisms as well as intracellular mechanisms (such as intracellular enzyme activation, calcium accumulation and heat shock protein activation).7 8 Increased calcium transients potentiate co-localisation of zymogen and lysosome granules and ultimately premature conversion of typsinogen to trypsin.9 Medications that may cause AP through acinar cell injury include azathioprine, corticosteroids and thiazide diuretics. Ethanol-induced pancreatitis has different pathophysiological mechanisms. Ethanol is directly toxic to the acinar cell, leading to inflammation and membrane destruction. There is also evidence that ethanol increases pancreatic ductal pressure favouring retrograde flow and intra-pancreatic enzymatic activation.10 It is likely that the ischaemia-reperfusion injury plays a role in the development of AP, which is supported by the importance of early aggressive fluid resuscitation.11 Microvascular changes may lead to increased pancreatic vascular permeability, oedema, haemorrhage and pancreatic necrosis. These hypotheses have led to detection of novel molecular therapeutic targets such as tumour necrosis factor -α and interleukin-6, both important activators of the inflammatory response in AP.12 A recent Cochrane review including 84 randomised controlled trials (RCTs) examined the efficacy of specific medical therapies in the treatment of AP; however, none of these showed clinical benefit or decreased short-term mortality over standard supportive treatment with intravenous fluids, electrolytes and organ support.13 As such, there does not appear to be any current role for specific, targeted medical interventions in the management of AP.
Diagnostic approach
The diagnosis of AP must be considered in any patient presenting with abdominal pain. History and examination can be indicative of AP ; however, two out of the following three criteria should be met for diagnosis:
Typical history.
Elevated serum amylase or lipase (>3 ULN).
Imaging (CT, MRI or ultrasound) consistent with acute pancreatitis.
History
A thorough history is required to determine the nature of the presenting abdominal pain, and for the presence of risk factors for pancreatic disease. Age and sex are important demographics because the two most common causes of AP differ. Gallstone pancreatitis is seen most commonly in patients with gallbladder disease, typically women over the age of 60, while alcoholic pancreatitis is seen more frequently in men, and generally at a younger age than those with gallstone pancreatitis.1 Metabolic, drug-related and procedural aetiologies should be considered. A history of previous AP should be documented. A family history is important to exclude hereditary pancreatitis and familial cancer syndromes. All medication, and in particular new medicines, should be reviewed.
The most common presenting pattern of pain is severe epigastric pain that radiates to the back, is exacerbated by movement and is alleviated by leaning forwards. Patients may appear agitated, confused and in distress. They may give a history of anorexia, nausea, vomiting and reduced oral intake.14 A history of symptoms in keeping with associated cholangitis should be sought.
Physical examination
Patients usually have signs of hypovolaemia and may appear diaphoretic, tachycardic and tachypnoeic. Fever may occur due to either cytokine release as part of the normal inflammatory response or may represent complicated pancreatitis, for example, pancreatic necrosis with or without infection. Reduced breath sounds and stony dull chest percussion suggest a pleural effusion, which may rarely be present on initial presentation although commonly develop as a later complication.15 The abdominal examination may reveal a tender and distended abdomen with voluntary guarding and with reduced bowel sounds if there is an associated ileus. Clinical signs of hypocalcaemia are rare but may be evident. Haemorrhagic pancreatitis is very rare and may cause ecchymoses of the periumbilical skin (Cullen’s sign), within the flanks (Grey-Turner’s sign) or over the inguinal ligament (Fox’s sign).16 Other important differentials of retroperitoneal haemorrhage include ruptured abdominal aneurysm and ruptured ectopic pregnancy.
Laboratory investigations
Routine blood tests including liver enzymes, triglycerides and calcium should be obtained. Elevations in creatinine and urea suggest acute kidney injury secondary to third space fluid loss and intravascular depletion. Haemoconcentration is associated with an increased risk of developing pancreatic necrosis. In the absence of choledocholithiasis, liver function tests are usually relatively normal. An elevated alanine aminotransferase (ALT) at presentation suggests a likely biliary origin. A meta-analysis found that an elevated serum ALT concentration of 150 IU/L or more within 48 hours of symptom onset had a positive predictive value of 85% in predicting a gallstone aetiology in patients with AP.17
Elevated levels of serum amylase or lipase (>3 ULN) support, but are not pathognomic for a diagnosis of AP. Conversely, amylase and lipase may not reach the diagnostic threshold in cases of AP; it is therefore necessary to have a low threshold for treating patients when there is a high index of suspicion. The diagnostic performance of these tests decreases in the hours and days after the onset of AP, and so additional investigations should be performed if there is suspicion of established AP. Early and serial C reactive protein testing is used in AP as an indicator of severity and progression of inflammation. Arterial oxygenation should be closely monitored and hypoxia treated with supplemental oxygen. Arterial blood gas sampling should be considered in order to assess both oxygenation and acid-base status.
Imaging
Radiographic studies are not used for diagnosis of AP, but may determine aetiology and exclude alternative diagnoses. A chest radiograph may show basal atelectasis and a pleural effusion. Abdominal radiograph may reveal a sentinel loop (isolated dilatation of a segment of gut) adjacent to the pancreas, demonstrate calcified gallstones (present in only 15%–20% of all cases with proven gallstones)18 or demonstrate pancreatic calcification as a feature of chronic pancreatitis.
Trans-abdominal ultrasound is the preferred initial study in suspected gallstone pancreatitis as it is inexpensive, available at the bedside and allows examination of the gallbladder and biliary tree. The sensitivity of conventional ultrasound in detecting AP is up to 75% but is limited by overlying bowel gas in 25%–30% of patients.19 Patients that become systemically unwell, septic or who do not improve should have a multiphase contrast-enhanced CT scan to rule out peripancreatic collections, necrosis, abscesses and vascular complications of pancreatitis (eg, development of portal venous thrombus, pseudoaneurysms or haemorrhage). Areas of reduced pancreatic parenchymal enhancement indicate pancreatic necrosis. While CT is the preferred initial modality for staging AP and detecting vascular complications, it is not advised within the first 48 hours of admission (unless there is diagnostic uncertainly) as this has been associated with increased length of stay, underestimation of the degree of pancreatic necrosis and with no improvement in patient outcomes.20 For serial examinations, MRI is gaining favour with the use of MR cholangiopancreatography (MRCP) sequences to detect/exclude aetiological factors (including biliary and pancreatic stones), improved depiction of the solid and liquid components of pancreatic and peripancreatic collections (thereby facilitating planning of drainage procedures), and better characterisation of pancreatic parenchyma including acute inflammation, residual volume and fibrotic change (from previous insults).21–23 Endoscopic retrograde cholangiopancreatography (ERCP) is only recommended acutely in cases of gallstone pancreatitis complicated by cholangitis. A meta-analysis found no evidence that early routine ERCP significantly affects mortality or morbidity in biliary pancreatitis other than in those patients with coexisting cholangitis or biliary obstruction.24 In patients considered to have idiopathic AP, after negative work-up for biliary aetiology, endoscopic ultrasound (EUS) should be considered to detect microlithiasis and cross-sectional imaging should be reviewed to exclude pancreatic neoplasm, particularly relevant in patients aged >50 years. A systematic review including 416 patients with idiopathic AP reported a 32%–88% diagnostic yield of EUS, detecting either biliary sludge or signs of chronic pancreatitis.25 If an EUS is normal, secretin stimulated MRCP may be considered to assess for rare anatomical abnormalities.26
Prognostication in AP
Several prognostic scores have been developed or adapted to predict disease severity. According to the International Association of Pancreatology and American Pancreatic Association (IAP/APA) guidelines, the presence of a systemic inflammatory response syndrome (SIRS) at admission and persistent SIRS at 48 hours both predict severe AP.26 Persistent SIRS was associated with a mortality of 25% compared with 8% for transient SIRS.27 The sensitivity of persistent SIRS for predicting mortality is 77%–89% and specificity 79%–86%27–29 and of SIRS at admission 100% and 31%, respectively.28 Other scoring systems do exist—such as APACHEII, Ranson and modified Glasgow score—but none of these are superior or inferior to (persistent) SIRS at predicting mortality.30
Treatment
The main goal of initial treatment is to alleviate symptoms and prevent complications by reducing pancreatic secretory stimuli and correction of fluid and electrolyte abnormalities. Initially, patients should be fluid resuscitated and kept nil by mouth with bowel rest when nausea, vomiting or abdominal pain are present. Supportive care continues until pain is resolved and diet restarted. The majority of patients will improve within 3–7 days of conservative management. Patients with organ failure or poor prognostic signs (persistent SIRS, Glasgow score >3, APACHE score >8 and Ranson score >3) should be assessed for admission to a high dependency unit.26
Initial resuscitation
Resuscitation with intravenous fluids, analgesics and antiemetics should form part of the initial treatment even before the diagnosis of AP is made. Goal-directed rehydration with Ringer’s lactate solution (or Hartmann’s) is recommended31 at a rate of 5–10 mL/kg/hour until resuscitation goals are reached.26 A recent triple-blind RCT compared Ringer’s lactate to normal saline in AP and found that Ringer’s lactate was associated with an anti-inflammatory effect which was attributed to the properties of lactate.32 A urinary catheter should be inserted in severe AP in order to record accurate fluid balance. Overly aggressive hydration leads to increased rates of sepsis, the need for more mechanical ventilation and higher mortality33 34; therefore, infusion rates should be carefully tailored to individual patients, taking into account factors such as age and comorbidities. Adequate early fluid resuscitation is the single most important aspect of the medical management, reducing organ failure and in-hospital mortality.35 Effective pain control is important in order to prevent diaphragmatic splinting, thereby reducing the risk of respiratory complications. The most commonly used drugs are opiates (morphine or fentanyl) either for breakthrough pain or as patient-controlled analgesia. Close monitoring of arterial oxygenation, acid–base balance and blood glucose should follow the intensive treatment modes of other critically ill patients.
Severe pancreatitis
The treatment of severe pancreatitis should be delivered in a high dependency unit. Insulin should be administered to maintain strict glucose control as this has been associated with reductions in morbidity and mortality in critical illness.36 Hypocalcaemia and hypomagnesaemia should be identified and treated to avoid the development of cardiac arrhythmias.
Antibiotics in AP
The use of antibiotics in non-infected pancreatitis is not currently recommended as there is no clear evidence of benefit. Prophylactic antibiotics have not been shown to reduce mortality, extra-pancreatic infections or the need for surgical intervention. A meta-analysis demonstrated no difference in the rates of infected necrosis, surgery or mortality between patients receiving antibiotics and those receiving a placebo for the treatment of severe AP.37 Some studies have shown a small benefit in cases of severe necrotising pancreatitis; therefore, antibiotic use should be restricted to patients in whom infection is strongly suspected.38 It is possible that injudicious use of antibiotics in walled off necrosis (WON) may lead to the development of resistant organisms once infection does develop.
Collections in severe pancreatitis
The management of pancreatic and peripancreatic collections has evolved over the past decade. The 2012 revised Atlanta criteria discern four types of peripancreatic fluid collections in AP depending on the content, degree of encapsulation and time (figure 1).

Atlanta classification of pancreatic fluid collections.39
Indications to drain pancreatic collections include infection and symptomatic sterile necrosis, while persistent collections that are asymptomatic may be observed. WON typically occurs >4 weeks after the onset of AP.39 Infected pancreatic necrosis should be diagnosed based on clinical signs and the presence of gas on imaging, fine needle aspiration is not routinely required.26 The choice and progression of intervention depends on individual patient factors including the anatomy of the collection and may involve an endoscopic or radiological approach. Open (surgical) necrosectomy is no longer recommended in necrotising pancreatitis following the landmark PANTER trial (Minimally Invasive Step Up Approach versus Maximal Necrosectomy in Patients with Acute Necrotising Pancreatitis) published in 2010 which showed that a minimally invasive step-up approach compared with open necrosectomy reduced the rate of major complication and death among patients with necrotising pancreatitis and infected necrotic tissue.40 In general, many patients are suitable for a ’step-up' approach, starting with conservative management and then to either percutaneous drainage or endoscopic transluminal drainage in selected patients within experienced high-volume endoscopic centres. Patients who do not respond to initial percutaneous or endoscopic drainage may require either upsizing to larger or more numerous percutaneous drains or endoscopic necrosectomy in those with an endoscopically placed lumen apposing metal stent (LAMS). A recent meta-analysis has indicated that patients with WON drained endoscopically with LAMS may do better than those drained with plastic stents.41 A large UK case series has demonstrated safety of LAMS in WON, in contrast to a series in the USA that showed a significant complication rate from LAMS.42 43 (In our practice, we favour endoscopic drainage with large diameter LAMS in cases of WON when anatomically favourable, and often insert a pigtail plastic stent through the LAMS to prevent solid debris blocking the LAMS and precipitating a septic episode. We image the patient at 4 weeks and remove the LAMS at that point. If the collection persists, we would consider retaining the patency of the tract with plastic pigtail stents.)
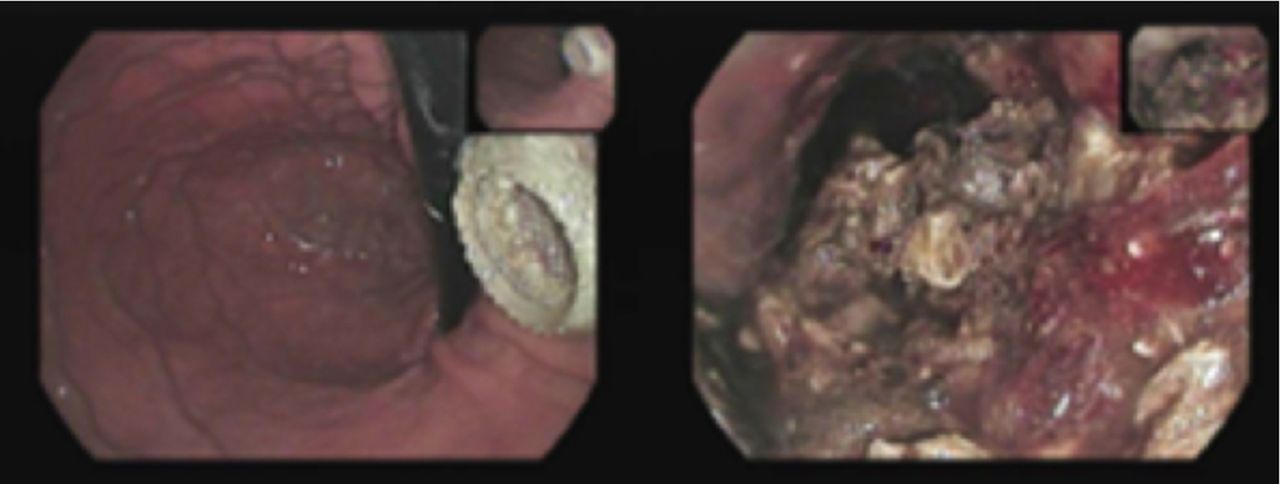
Pseudocysts may resolve spontaneously; however, do require drainage in the case of complications (infection, biliary or duodenal obstruction) or if the patient is symptomatic with pain. Endoscopic cystgastrostomy with multiple plastic pigtail stents is the preferred drainage option although percutaneous drainage may be considered in unfavourable anatomy. The use of LAMS for the drainage of pseudocysts is well described for ease, but the risks, clinical benefit and cost implications have not yet been studied. The timing and choice of approach requires multidisciplinary collaboration. Figure 2 demonstrates CT findings in AP, and figure 3 demonstrates the endoscopic view of a LAMS alongside an endoscopic necrosectomy.

CT findings in acute pancreatitis. Top left: acute interstitial pancreatitis; post-contrast portal venous phase axial CT image through the pancreas. The pancreas enhances homogeneously but there is ill-defined peripancreatic fat stranding centred on the head and body of the pancreas (white solid arrows) extending to involve the tail (white clear arrow). Note a small volume of free fluid in the lesser sac (interposed between the head of the pancreas and gastric antrum) and in the hepatorenal space. Top right: pancreatic pseudocyst; post-contrast portal venous phase axial CT image through the pancreatic tail. At this stage, acute inflammation has settled but there is a well-defined fluid density cystic lesion in the tail of pancreas (white solid arrow), with normally enhancing pancreatic tissue on either side of the lesion. Bottom left: acute necrotic collection; post-contrast late arterial phase axial CT image through the pancreas. Note patchy areas of pancreatic parenchymal hypoenhancement in the posterior head and tail of pancreas (white solid arrows). There is ill-defined peripancreatic fat stranding with free fluid crossing between retroperitoneal and peritoneal compartments, involving intra-pancreatic and extra- pancreatic tissues. Bottom right: early walled off necrosis ; post-contrast portal venous phase axial CT imaging through the pancreas. At this stage, ill-defined peripancreatic collections that cross between anatomical compartments are seen to become more organised with thick enhancing walls (solid white arrows) and heterogeneous internal debris (eg, fat density components, white clear arrow).

{kind=link}
{kind=link}
{kind=link}
Endoscopic image of lumen apposing metal stent (left) and endoscopic necrosectomy (right).
Nutrition
In cases of mild pancreatitis, enteral nutrition should be recommenced as soon as abdominal pain has subsided.44 In severe pancreatitis, patients should be kept nil by mouth until fully resuscitated, usually after 48 hours, at which point normal enteral diet (if tolerated) or enteral tube feeding should be commenced.26 Two meta-analyses have demonstrated that enteral nutrition, compared with parenteral nutrition, decreases sepsis, organ failure, the need for surgical intervention and mortality.45 46 Post-pancreatic feeding is no longer recommended unless there is mechanical gastric outlet obstruction or the patient is unable to tolerate nasogastric tube feeding.47 Parenteral nutrition should be reserved for patients who are unable to reach nutritional goals with nasojejunal feeding. A delay of up to 5 days in the initiation of parenteral nutrition may be appropriate to allow for restarting of oral or enteral feeding.26 Pancreatic enzyme supplementation should be prescribed to patients with symptoms of pancreatic exocrine insufficiency.48
Alcohol-induced pancreatitis
Patients with alcohol-induced pancreatitis may need alcohol-withdrawal prophylaxis. Benzodiazepines, thiamine, folic acid and multivitamins are generally used. Dedicated outpatient follow-up visits are advised to prevent recurrence.49
Gallstone pancreatitis
All patients presenting with gallstone pancreatitis should be considered for cholecystectomy when they are well enough to undergo surgery. In cases of mild biliary pancreatitis, cholecystectomy should ideally be performed during the index admission or within 2 weeks of discharge as interval cholecystectomy is associated with a significant risk of readmission for recurrent biliary events.26 A systematic review found an 18% readmission rate for recurrent biliary events a medium of 6 weeks after index admission for mild gallstone pancreatitis.50 In cases of severe gallstone pancreatitis, cholecystectomy may need to be delayed until collections have improved, unless the patient is well enough for surgery and the gallbladder is some distance from the collection.26 In surgically unfit or frail elderly patients, ERCP with biliary sphincterotomy may be considered as definitive treatment although the risks of sphincterotomy should be balanced against the risk of recurrent biliary events.51
Prognosis
Most patients with AP will improve within 1 week of conservative management and be well enough for discharge. The aetiology should be identified, and a plan to prevent recurrence should be initiated before hospital discharge. Long-term prognosis is based on the aetiological factor and patient compliance to lifestyle modifications. AP generally resolves and leaves pancreatic function intact. Many patients progress to recurrent AP or chronic pancreatitis, and the risk is higher among smokers, alcoholics and men.
NCEPOD report (2016)
In 2016 the National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) published a report into the care of patients with AP within the National Health Service. Overall 45% of patients received ‘good practice’, room for improvement was identified in 52% and 3% of patients had ‘less than satisfactory care’. Key areas for improvement were better documentation of physiological parameters and early warning scores, increased multidisciplinary input to manage comorbidities, accurate assessment of nutritional risk, simplified rapid referral pathways for ERCP and timely cholecystectomy in patients with biliary pancreatitis. In addition, it concluded that all patients with severe AP requiring radiological, endoscopic or surgical intervention should be managed within a specialist tertiary referral centre. The report found an overall mortality of 13% in AP and recommended that all deaths are discussed in morbidity and mortality meetings with learning shared through network meetings.52
References
Footnotes
Contributors All authors contributed equally to this review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no unpublished data in this article.