Article Text

Abstract
Hippocrates noted that “it is a general rule, that intestines become sluggish with age”, though the precise mechanisms for this association remains uncertain even today.
- constipation
- autonomic nervous system diseases
- nervous system
- gastrointestinal motility
- PD, Parkinson’s disese
- MSA, multiple system atrophy
- MS, multiple sclerosis
Statistics from Altmetric.com
Many neurological and psychiatric disorders are associated with constipation,1 and this paper is a review of the current clinical knowledge regarding the pathogenesis and clinical findings. We will comment on the location of lesions, the possible pathogenesis of the symptoms, and the treatment of constipation, within a number of different neurological diseases. This field is rapidly expanding, as a better understanding of the physiology of bowel movements and defecation is achieved. The main focus is on idiopathic Parkinson’s disease and other parkinsonian syndromes where the mechanism of constipation seems to be a result of a genuine autonomic failure.
ANATOMY AND PHYSIOLOGY OF THE COLON AND DEFECATION
The physiology of the colon is complex and modulated through several separate systems, including neural, endocrine, and luminal factors. The neural control can be separated into the intrinsic colonic nervous system and the extrinsic colonic nervous system. The intrinsic nervous system consists of nerve cell bodies and endings that are located between the circular and the longitudinal muscle coats.
The intrinsic nervous system of the colon consists of neurons, with cell bodies in the submucosal ganglia (Meissner’s plexus) and the myenteric ganglia (Auerbach’s plexus), which are interconnected through interneurons and act as single functional units.2, 3 The classification of the intrinsic colonic neurons is very complex, as numerous neurotransmitters have been located and identified. However, the physiological role of each and the combination of these are not yet clear.
The extrinsic colonic nervous system innervates the gut, and presumably acts as a modulator of visceral activity through sympathetic and parasympathetic functions.
The parasympathetic innervation of the colon is divided into cranial (vagus nerve) and sacral (pelvic nerves S2–4) divisions. The vagus nerve innervates the foregut and midgut (ending at the splenic flexure) and the pelvic nerves innervate the hindgut (descending and sigmoid colon and the anorectum). Stimulation of parasympathetic fibres increases the overall activity of the gastrointestinal tract by promoting peristalsis, and increasing local blood flow and intestinal secretion, and this system is also an integral component of the defecation reflex.
The sympathetic innervation of the gastrointestinal tract originates in the thoracolumbar outflow (T5-L2), and it works by the inhibitory effect of noradrenaline on the enteric nerves. Contraction of the internal anal sphincter is responsible for the resting anal pressure, and is probably regulated by the sympathetic nervous system.3, 4
The external sphincter is innervated via branches of the pudendal nerves (S2,3,4) as is sensation from the perianal area and perineum, whereas tension and stretch in the rectal wall and proximal part of the anal canal is carried in the pelvic nerves. In the central nervous system, the medial prefrontal area and the anterior cingulate gyrus seem to represent two important higher centres that contribute to the regulation of bowel function, and are involved in the timing and initiation of defecation with their effects over voluntary control being mediated through spinal pathways.
Before defecation, faecal material stored in the colon is propelled past the rectosigmoid sphincter, a so called “physiological sphincter”, into the normally empty rectum by colonic mass movements. Distension of the distal rectum initiates afferent signals that are associated with a sensation of need to defecate.5 If it is judged to be appropriate, a final series of neurologically controlled events are initiated and defecation occurs. Using Valsalva straining, an increase in intra-abdominal pressure is produced, which is followed by pelvic floor descent, and the rectoanal inhibition reflex is started. The rectoanal inhibitory reflex results in internal anal sphincter relaxation and a voluntary relaxation of the external sphincteric and pubococcygeal muscles. Defecation can be delayed by contraction of the external anal sphincter and the urge to defecate gradually decreases in intensity over a period of minutes.4
GENERAL CONSIDERATIONS ON CONSTIPATION
According to the most used definition, constipation is evacuation of faeces less than three times a week, and one study have demonstrated that diaries may be a safe way to evaluate frequency and/or consistency.6, 7 It may be argued, that only objective means of evaluating the patients are valuable; colonic radiography, measuring colon transit time, and anal-sphincter manometry and/or sphincter EMG. These considerations are conflicting, but the most operative measure used both in daily practice and to include patients in clinical studies is the frequency, and the most widely accepted investigation to diagnose constipation is radiography with radio-opaque markers,8 though specificity and sensitivity is difficult to assess.9, 10
Outlet obstruction type of constipation in the neurological diseased person is mainly attributable to an inability to relax the pelvic floor and to reduce the anorectal angel, and is thereby a functional obstruction, in contrast with obstruction attributable to neoplasia and other causes to stenosis. When the puborectalis muscle fails to relax or even contracts during defecation, the forward passage of faeces is obstructed. Paradoxial contraction of the external sphincter may occur as well.11 Patients, who have difficulty in evacuating the rectum, generally have outlet obstruction, and constipation occurs because the faeces harden in the rectum causing faecal impaction. This acts like a mass causing abdominal discomfort, bleeding, and “overflow” incontinence (stercoral diarrhoea), when liquid stool bypasses the hard mass in the colon, symptoms which may be seen in any constipated patient.
CONSTIPATION IN THE GENERAL POPULATION
The prevalence of constipation in the population is comparatively high; around 15%, with a higher prevalence in the female population and in elderly people.12 In one study investigating almost 15 000 women, 14% to 27% were found to be constipated, highest prevalence in elderly people.13 Walking less than 0.5 km a day increases the risk of constipation in elderly people,14 but the role of exercise in the treatment has been challenged.15, 16 There seems to be strong beliefs, within both medical professionals and the general population that dietary fibre intake should be around 35 g of fibre a day, and it has been documented, that this volume increases the frequency of defecation.17, 16 Reports are not unanimous in respect of preventing or changing the course of constipation with dietary fibre,18, 19 and the beneficial effects in treatment in neurological diseases are not evident.
1 CONSTIPATION IN DISEASES MAINLY AFFECTING THE BRAIN
In the neurological diseases affecting the central nervous system, the intrinsic nervous system seems to remain intact and functional, while some modulation in the extrinsic nervous systems occurs.
A Constipation in stroke
Constipation and stroke seems associated, yet no studies have been able to show a direct association either clinically or pathophysiologically.18 However, the number of studies in this field is limited. It is a general experience, that constipation is frequent in acute admitted stroke patients. There may be several explanations for this: the patients are elderly, often treated with a number of drugs, dehydrated, and immobile already at admittance. Box 1 lists a number of drugs, which themselves or in combination may induce constipation. Bed rest and immobility often give rise to constipation, and may in addition induce deconditioning, resulting in inadequate force to defecate.
Hypovolemia is a common problem, both before and after stroke, the latter as a result of dysphagia and/or impaired thirst mechanisms and lack of attention to drinking possibilities. Diet may be another problem, as the hemiplegic population often has an insufficient intake of dietary fibre.
Lesions affecting the pontine defecatory centre may disrupt the sequencing of sympatical and parasympathical components of defecation, and impair the coordination of the peristaltic wave and the relaxation of the pelvic floor and external sphincter.18
1 Box 1
A number of drugs are themselves or in combination able to induce or aggravate constipation and the list of drugs should always be evaluated carefully in the constipated patient. This box summarises the drugs most frequently used.
-
Diuretics
-
Iron
-
Antihypertensives
-
Antipsychotics
-
Aluminium and calcium containing antacids
-
Anticholinergics
-
Anticonvulsants
-
Opioid analgesics
-
Ganglionic blockers
Stroke syndromes can in addition to paresis and speech problems result in cognitive problems, object agnosia, visuospatial desorientation, or attention disturbances, resulting in impaired ability to defecate at a socially accepted time and place, and in constipation. However, the establishment of dedicated stroke units with early mobilisation, safe rehydration, and diet regulating measures have resulted in a considerable reduction of the problems with constipation in stroke patients and hence in a lower morbidity and probably reduced mortality, though the coherence of the latter issue is subject to debate.
B Constipation in parkinsonian syndromes
James Parkinson recognised gastrointestinal features in his original monograph published in 1817.20 Gastrointestinal dysfunctions is a frequent and occasionally dominating symptom of Parkinson’s disease (PD), and include drooling, dysphagia, gastroparesis, and constipation as a result of decreased bowel movement frequency, and defecatory dysfunction resulting in incomplete evacuation.
Numerous studies have established that the prevalence of constipation in PD is very high. More than 50%21, 22 (in one study as high as almost 80%23) of Parkinson patients suffer from moderate to severe constipation,24, 25 and this frequency is significantly higher than in controls.
The pathophysiology of constipation in PD seems to be multifactorial. Lewy bodies have been found in both parasympathetic nuclei and nerves, including the vagal nucleus and myenteric plexus from upper oesophagus to rectum,26, 27 indicating a genuine autonomic failure with a pathoanatomical basis. This is consistent with neuropathological studies, in which histological changes were found in the corresponding areas28, 29 with Lewy bodies in both CNS as well as degeneration and depletion of dopaminergic neurones of the myenteric and submucosal plexus27, 30, 31
Several studies have been conducted to establish, to what extent decreased bowel movement and defecatory dysfunction contributes to the symptoms. Jost et al32 found, that 28% of de novo patients showed signs of neurogenic abnormalities in sphincter EMG, whereas 24% had pathologically prolonged colon transit time evaluated by radiography. Severe constipation, which is often resistant to treatment, may occur before the first symptoms of parkinsonism appear.33 It is possible however, that these studies have included a substantial number of patients with multiple system atrophy (MSA), as autonomic dysfunction is a prominent feature in MSA and neurogenic changes in sphincter EMG are believed not to be a common finding in early PD.
Antiparkinsonian medication often has a direct action on gastric activity. Anticholinergic agents have been stated to delay transit time, but this seemed not to be the case in the paper by Edwards and coworkers from 1991.25 As Levo-dopa (l-dopa) is activated to dopamine in the lumen of both the stomach and the small and large bowel, it may be hydroxylated to noradrenaline, which slows bowel movements. This may lead to heterogeneous absorption, which in turn contributes to motor fluctuations, leading to an increased use of l-dopa, and thereby start an unfortunate circle of actions. Studies have shown, that if the constipation in PD is treated, the blood concentrations of l-dopa are increased, and fluctuates less, although an improved gastric emptying may also play a part through the gastrocolic reflex,34, 35 but no randomised placebo controlled studies are available. Studies have indicated that dopamine itself prolongs gastrointestinal transit time in healthy volunteers.36 However, constipation in PD was known long before specific treatment was found.20 Studies on dopamine receptor agonists suggest that constipation may be more frequent in the group receiving these than in the placebo group, though these problems seems to improve significantly as treatment is continued for more that 10 weeks (www.mdconsult.com 2001).
The lack of physical exercise as a symptom of PD is obviously a contributing factor as well as a reduced intake of fibre and water because of chewing problems (bradykinaesia) and dysphagia.
A number of studies using anorectal manometry have revealed several abnormalities in patients with PD and other parkinsionian syndromes,37, 38 including low basal and impaired squeeze pressure, phasic fluctuations during squeeze, and a hypercontractile response to rectosphincteric reflex. One study has indicated, that these changes may be responsive to antiparkinson medication.37 Hence, medication may be both working provocative and improving on constipation in PD.
Most studies on MSA and its autonomic features relate to bladder dysfunction, and the literature specifically on constipation is limited. A number of earlier studies on PD and constipation may have included patients with MSA, but the true prevalence is not known.38 However, studies also indicate that fecal incontinence is a frequent problem in MSA. Studies have not found any significant differences in complaints or in anal physiology between PD and MSA,38, 49 besides abnormal anal sphincter EMG, which may be helpful in order to differentiate the two conditions in early stages.40
There are no papers published on constipation in either generalised dystonia or Huntington’s chorea.
2 CONSTIPATION IN DISEASES ALSO AFFECTING THE SPINAL CORD
A Constipation in multiple sclerosis
Bowel dysfunction in patients with multiple sclerosis (MS) is common. Constipation and faecal incontinence often coexist and occur in 39% to 73% of MS patients, depending on definitions and selection.41, 42
The pathophysiology of bowel dysfunction in MS is poorly understood. Symptoms of bowel dysfunction are not nearly as frequent as bladder dysfunction,43 indicating a more complex mechanism than the result of spinal lesions. Abnormalities of colonic activity and slow transit time have been demonstrated in patients with MS.43, 44 A pathoanatomical explanation of slowed transit time is unidentified, and Clare Fowler has suggested, that the symptom of constipation could be a mechanism similar to that which causes fatigue in MS.45
In respect to faecal incontinence, Nordenbo et al found a strong correlation between impaired rectal sensation and incontinence,46 and many patients may either clinically or manometrically have poor voluntary squeeze pressure, and may start the anorectal inhibitory reflex earlier than controls.
Patients with severe paraparesis may complain of difficulty in “switching on” the mechanism of defecation.45, 47 Spasticity of the pelvic floor is associated with a failure of effacement of the puborectalis during attemps to empty the rectum, and patients may find digitation necessary to assist evacuation.45, 47
B Constipation in spine and spinal cord disorders and cauda equina
An important and time consuming problem in caring for patients with spinal cord injury is constipation, and the presence of this is well documented.48, 49 It is known that the mechanism of constipation in spinal cord injured patients is prolonged colonic transit time,50, 51 but the pathophysiological background for this is still not known.48
In the patient with spinal cord injury, the extrinsic neural control is lost, and patients with spinal cord lesions demonstrate disordered sympathic function. The nature of this abnormality depends on the level and the degree of the lesion, and is often clinically evident in relation to gastrointestinal function. Impairment is generally most pronounced in patients with quadriplegia with a complete transection above the sympatic outflow.48, 52
In high cord transection with intact isolated cord below the lesion, resting colon activity is reduced compared with normal controls, whereas patients with low cord lesions show a significant increased colonic activity.5 It has been concluded from these findings, that an inhibitory centre in the lumbar outflow exists, and that in patients with low cord injury, this outflow is inhibited, resulting in increased sigmoid activity.52
By these mechanisms both constipation and incontinence exist in spinal cord injury.
Patients with cauda equina lesions may have an atonic bowel and develop severe and chronic constipation, and they often suffer from overflow incontinence. This is believed to be a result of parasympathetic denervation of the rectum and sigmoid, combined with denervation of anal sphincters. In the development of the acute cauda eqiuna lesion, anal incontinence is a key symptom, and as possible causes are numerous, this symptom in combination with sensory disturbances, leg weakness, and absent tendon reflexes must not be ignored, as early neurosurgical intervention is needed to reverse the symptoms.51
3 CONSTIPATION IN DISEASES AFFECTING THE PERIPHERAL NERVOUS SYSTEM AND MOTOR NEURONES
Bowel symptoms, as a sign of peripheral nerve damage are seen in generalised as well as pure autonomic neuropathies. The most frequent observed condition is diabetic neuropathy, in which constipation will not be the only symptom, as other peripheral signs will be present. Most patients will complain of alternating diarrhoea and constipation, as both conditions seems to occur more often in the diabetic population than in a background population,53, 54 although a recent larger study have not found this difference.55 There is no difference in prevalence between IDDM (type I) and NIDDM (type II), and there are conflicting reports of whether an association between symptoms of decreased colonic transit time and the presence of peripheral or autonomic neuropathy exists.56 The pathophysiology of constipation in diabetes is unclear, but it may be attributable to (1) direct complications of autonomic neuropathy, (2) indirect complication of autonomic neuropathy (bacterial overgrowth), and (3) a manifestation of the underlying diabetes (dysmotility attributable to hyperglycaemia).56 Histopathological studies of the vagus nerve in patients with diabetes and gastrointestinal manifestations have revealed reductions in the number of unmyelinated fibres, indicating a component of autonomic dysfunction in these symptoms.57
In familial amyloid neurophathy, uncoordinated contractions of the small bowel have been demonstrated, mainly resulting in diarrhoea, but constipation may be alternating with diarrhoea, whereas in primary amyloidosis diarrhoea and steatorrhoea are prominent.
In acute porphyria, constipation, abdominal pain and sometimes vomiting are frequent gastrointestinal symptoms. The porphyries that present with these symptoms (variegate porphyria, acute intermittent porphyria, and hereditary coproporphyria) are the ones also associated with peripheral neuropathies, suggesting a role for autonomic neuropathy in the symptomatology.56
In paraneoplastic dysautonias originating from small cell and bronchial lung cancers, Hodgkin’s disease, and breast cancer, constipation, and pseudo-obstruction is frequently seen as a sign of postganglionic autonomic neuropathy56 and it may even be a presenting feature.58, 59
In myotonic dystrophy constipation is relatively uncommon,53 as most patients suffer from diarrhoea and abdominal cramps. Megacolon and abnormalities in manometric evaluation attributable to abnormal and sustained contraction of both internal and external sphincters have been demonstrated, and case reports have documented smooth muscle involvement.60, 61
Constipation as well as diarrhoea may be features in most muscular dystrophies, but this has only been investigated systematically in Duchenne’s dystrophy, where colonic transit time is increased, and cases of psuedo-obstruction have been encountered.53 It has been suggested that in such cases there is significant atrophy and fibrosis of the intestinal smooth muscles.
Constipation as a result of the neurological condition in itself is rarely seen in amyotrophic lateral sclerosis.62 As swallowing difficulties are prominent in amyotrophic lateral sclerosis, fluid intake may be restricted and exercise is limited, these patients may often be constipated.
Onuf’s nucleus innervating the external sphincters seems to be spared for a long time in amyotrophic lateral sclerosis, but degenerative patterns have been demonstrated in both EMG and in pathology studies.63, 64
EVALUATION AND TREATMENT OF CONSTIPATION IN NEUROLOGICAL DISEASES
In evaluation of the neurologically diseased patient with respect to gastrointestinal dysfunction, a combination of a carefully taken history (for example, using diaries), including actual medication, and physical examination including digital exploration, will be adequate in most cases. Patients may present with abdominal discomfort or pain, and investigations generally do not detect any abnormalities. Based on history alone, it may prove to be difficult to differentiate slow colonic transit time and outlet obstruction. Severe cases of constipation secondary to slow colonic transit, may present with decreased appetite and not uncommonly with nausea, but rarely with vomiting.
Stercoral diarrhoea is a bothersome symptom and though the impaction is evident to the physician, it may prove difficult to treat.
Patients, who have difficulty in evacuating the rectum, generally have outlet obstruction and neoplasia needs to be excluded.
In female patients with severe constipation and difficulty with defecation, it is important to exclude rectoceles, which are mostly asymptomatic but sometimes can cause incomplete emptying.
Further investigation with radiography or manometry depends on the situation. In cases with incomplete emptying, manometry with anal sphincter EMG should be conducted to establish the reason for the prolonged straining.
It is reasonable to suspect a neurogenic cause of symptoms when constipation arises in any neurologically diseased patient, but the positive predictive value of constipation when suspecting neurological disease in an otherwise asymptomatic person is very low. However, studies have suggested that in otherwise healthy patients with constipation attributable to slow transit, a genuine autonomic dysfunction may be the cause, but these patients are not clinically distinguishable from patients constipated because of pelvic nerve damage from childbirth or surgery.65
The most widely used and accepted method of investigating constipated patients is the radio-opaque method.10, 24 This is an effective and simple test, although it is not able to detect the pathophysiological background for the prolonged transit time.23
The importance of conducting a multidisciplinary assessment to identify and minimise all the difficulties related to bowel dysfunction has often been emphasised.66 Careful planning of bowel regimen includes a number of other strategies rather than one single intervention; attention to diet, intake of fluids, bowel habits, evacuation techniques, and use of medication is important and with this, most patients will be able to achieve adequate evacuation.
Tradition in different countries plays a significant part in choice of treatment and considering the number of patients affected and variety drugs available, the number of placebo controlled studies is low.67, 68
Different approaches are indicated for different types of constipation. Bulk forming laxatives may be useful for those on an inadequate oral diet and to soften stools. However, the use of bulking agents may be counterproductive if peristalsis is impaired, and may add to the tendency to impaction, particularly in the immobilised patient. Stool softeners may help when the problem is difficulties in evacuation, and stimulants may help with slow transit. Extreme caution is needed if treating the suspected faecally impacted patient with stimulants. Table 1 summarises the most widely used preparations used in the treatment of constipation.
A comparatively large number of drugs and agents are available to treat constipation. This table lists some of them; see text for details on the use of prokinetic drugs. Most patients have tried a number of strategies before consulting the physician, including enemas
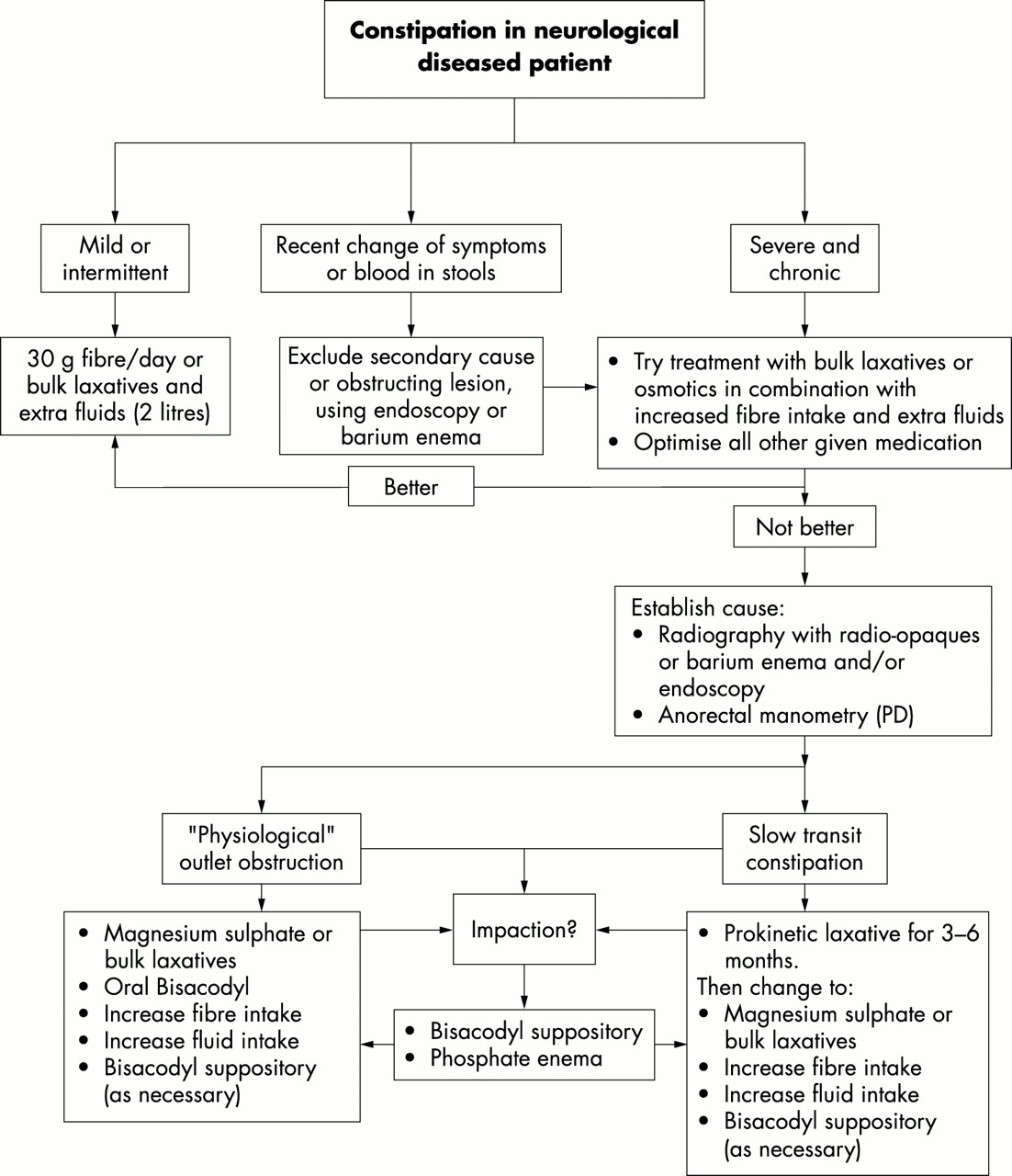
Figure 1 outlines a possible strategy for management and drug treatment in constipated patients.
{kind=link}
An algorithm of management of the constipated neurological diseased patient. Ruling out neoplasia is important in the patients who never previously have experienced constipation. Treatment of impaction is needed before treatment using bulk increasing laxatives is started. The need of extra fluids should be emphasised.
One study has found that senna fibres are more efficient than lactulose in increasing bowel frequency, improving stool consistency, and easing evacuation in older people.69 The need for extra fluid when taking bulk laxatives is often ignored but should be emphasised. Extra fluids are also needed, when treating constipation with magnesium sulphate, because of the risk of hypermagnesaemia resulting in renal failure.
In treating the constipated patient, a systematic approach is needed but rarely seen.70 Many interesting manoeuvres have been tried, the latest, visual biofeed back has not proved to be better than training toilet habits in improving constipation.71, 72
The use of “non-pharmacological” treatment, such as psyllium and other fibre rich diets, is widely used in the population, and most patients have tried bulk increasing agents and even enemas before consulting the physician.
If the patient has faecal impaction, enemas or digital evacuation, or both, can be the only solution. Again, many strategies have been tried73; and clinical investigation to rule out neoplasia is important, and establishing the right diagnosis is essential as outlined in figure 1. Once the impaction has been treated, preventing relapse is important, but no randomised studies are available. Training toilet habits by planning defecation into daily routines seems to be effective, and when daily exercise and bulk increasing or softening laxative is added, it is our experience that patients are well for some time. However, in the neurologically diseased patient, physical activity is often limited because of the condition.
A specific problem is treating the constipated PD patient. Medication may be a contributing factor, and it should be emphasised, that once antiparkinsonian treatment is optimised, the problem of constipation might have passed. As increased transit time is often the problem in PD, prokinetic drugs such as cisapride may show useful, as evaluated by Jost el al,74, 75 but the duration of this treatment is limited to three to six months because of possible side effects.76 Cisapride may be an efficient way of limiting motor fluctuations,34 and in further treatment and prevention, psyllium has proved useful in an open labelled study.77 The treatment of motor symptoms and of constipation in PD is thereby inseparable.
There are no published studies on the effect of medication on bowel symptoms in MS, in most cases the patients are willing to try laxatives as lactulose and magnesium oxide, as well as an enema in the morning. However, little can be offered to constipated patients with MS. Behavioural treatment (biofeedback) seems to have some effect in patients with limited general disability,72 but long term effects are unknown.
Treating constipation in spinal cord patients can be troublesome. Some authors recommend use of stool softening laxatives (preferably given as suppository), as both tradition and experience indicate an effect, but no blinded or placebo controlled studies are available, apart from one study in which no effect of cisapride52 on total transit time was found. Some patients may need a colostomy if pharmacological treatment fails.
CONCLUSIONS
Constipation is a frequent sign and complication in neurological diseases, and may be very troublesome to the patient if not treated early, and if relapse is not prevented. The physiology of the gut and the pathophysiology of constipation is very complex, and as the bowel function is mostly autonomic, the possibilities of specific treatment are limited. Many drugs may have an effect, but remarkably few double blinded, placebo controlled studies have been performed.
New JNNP online submission and review system
The Editors of JNNP are pleased to inform authors and reviewers of its new online submission and review system. Bench>Press is a fully integrated electronic system which uses the internet to allow rapid and efficient submission of manuscripts, plus the entire peer review process to be conducted online.
Authors can submit their manuscript in any standard word processing software. Graphic formats acceptable are: .jpg, .tiff, .gif, and eps. Text and graphic files are automatically converted to PDF for ease of distribution and reviewing purposes. Authors are asked to approve their submission before it formally enters the reviewing process.
To access the system click on “SUBMIT YOUR MANUSCRIPT HERE” on the JNNP homepage: http://www.jnnpjnl.com/, or you can access Bench>Press directly at http://submit-jnnp.bmjjournals.com/.
We are very excited with this new development and we would encourage authors and reviewers to use the on-line system where possible. It really is simple to use and should be a big improvement on the current peer review process. Full instructions can be found on Bench>Press http://submit-jnnp.bmjjournals.com/ and JNNP online at http://www.jnnpjnl.com/. Please contact Natalie Davies, Project Manager, ndavies{at}bmjgroup.com for further information.
PRE-REGISTER WITH THE SYSTEM
We would be grateful if all JNNP authors and reviewers pre-registered with the system. This will give you the opportunity to update your contact and expertise data, allowing us to provide you with a more efficient service.
Instructions for registering
-
Click on “Create a New Account” in the upper left hand side of the Bench>Press homepage
-
Enter your email address in the space provided.
-
Please be sure to enter the email address that you received this email message at. You will be given the opportunity to change this once you have created an account.
-
Choose a password for yourself and enter it in the spaces provided.
-
Complete the question of your choice to be used in the event you cannot remember your password at a later time.
-
Click on the “Save” button at the bottom of the screen.
-
Check the e-mail account you registered under. An email will be sent to you with a verification number and URL.
-
Once you receive this verification number, click on the URL hyperlink and enter the verification number in the relevant field. This is for security reasons and to check that your account is not being used fraudulently.
-
Enter/amend your contact information, and update your expertise data.