Article Text

Abstract
Objective To summarise currently reported neonatal cases of SARS-CoV-2 infection.
Methods A search strategy was designed to retrieve all articles published from 1 December 2019 to 12 May 2020, by combining the terms ‘coronavirus’ OR ‘covid’ OR ‘SARS-CoV-2’) AND (‘neonat*’ OR ‘newborn’) in the following electronic databases: MEDLINE/Pubmed, Scopus, Web of Science, MedRxiv, the Cochrane Database of Systematic Review and the WHO COVID-19 database, with no language restrictions. Quality of studies was evaluated by using a specific tool for assessment of case reports and/or case series.
Results Twenty-six observational studies (18 case reports and 8 case series) with 44 newborns with confirmed SARS-CoV-2 infection were included in the final analysis. Studies were mainly from China and Italy. Half of neonates had a documented contact with the infected mother and one out of three infected neonates was admitted from home. Median age at diagnosis was 5 days. One out of four neonates was asymptomatic, and the remaining showed mild symptoms typical of acute respiratory infections and/or gastrointestinal symptoms. The majority of neonates were left in spontaneous breathing (room air) and had good prognosis after a median duration of hospitalisation of 10 days.
Conclusions Most neonates with SARS-CoV-2 infection were asymptomatic or presented mild symptoms, generally were left in spontaneous breathing and had a good prognosis after median 10 days of hospitalisation. Large epidemiological and clinical cohort studies, as well as the implementation of collaborative networks, are needed to improve the understanding of the impact of SARS-CoV-2 infection in neonates.
- neonatology
- therapeutics
Data availability statement
Data are available on reasonable request.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
What is already known on this topic?
Recent reviews have provided an overview of published information on paediatric patients with SARS-CoV-2 infection, while data on infected neonates have been limited.
Given the severity of the pandemic and the low incidence in children, a review focusing on infected neonates could provide a more informative picture to health caregivers involved in the management of neonates with SARS-CoV-2 infection.
What this study adds?
Most neonates with SARS-CoV-2 infection were asymptomatic or presented mild symptoms, generally were left in spontaneous breathing and had a good prognosis.
Introduction
The COVID-19 pandemic continues to expand worldwide. At the time of drafting this paper (21 May 2020), almost 5 million confirmed cases of COVID-19 have been reported worldwide, with over 300 000 deaths.1
COVID-19 contagion is mainly through respiratory droplets or direct contact with infected subjects or contaminated surfaces.2 In neonates, vertical (intrauterine) transmission has also been postulated,3 4 but available evidence is insufficient to support this hypothesis.5 6
Available literature suggests that paediatric population may be less affected from COVID-19 than adult population.7 8 However, infants (children under 1 year) seem to be more vulnerable to SARS-CoV-2 infection with a higher severity of illness compared with other paediatric ages.9
Recent reviews have provided an overview of published information on paediatric patients with SARS-CoV-2 infection,10 11 while data on infected neonates has been limited, and no systematic reviews are available for newborns. Given the severity of the pandemic and the low incidence, a review focusing on infected neonates could provide a more informative picture to health caregivers involved in the management of neonates with SARS-CoV-2 infection.
This systematic review summarises currently reported neonatal cases of SARS-CoV-2 infection in order to offer an overview of clinical findings, diagnostic tests, management and prognosis of such vulnerable population.
Methods
Study design
Search strategy
This is a systematic review of observational studies describing neonates with SARS-CoV-2 infection between December 2019 and May 2020. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guideline.12
To identify relevant studies, we systematically searched MEDLINE/PubMed, Scopus, Web of Science, MedRxiv, the Cochrane Database of Systematic Review and the WHO COVID-19 database between 1 December 2019 and 12 May 2020. Two researchers (MEC and MB) independently reviewed search results and screened titles/abstracts. A third researcher (DT) resolved any inconsistency. We obtained the full texts of all potentially eligible studies. In PubMed, the following search strategy was used: (‘coronavirus’ OR ‘Covid-19’ OR ‘SARS-CoV-2’) AND (‘neonat*’ OR ‘newborn’). This search strategy was adapted to suit the other electronic sources. No language restrictions were applied. The reference lists of included articles were hand-searched to identify additional studies of interest.
Criteria for considering studies for this review
Observational studies describing neonates (babies younger than 28 days) with SARS-CoV-2 infection were considered eligible for this review. SARS-CoV-2 infection was defined as the presence of a positive nasopharyngeal or anal swab and/or the presence of high levels of IgM.13 Only the most recent and complete data were included when duplicate publications reporting on similar patients were found. Studies not including humans were excluded.
Data collection
Two researchers (MEC and SC) independently extracted key data from the included studies. A third researcher (FC) checked the extracted data. For each study, we retrieved relevant data on study characteristics (ie, first author, month/year of publication and study design), demographics (ie, sex and gestational age), diagnosis, laboratory data (ie, white cell count and platelet count), clinical characteristics (ie, symptoms), treatment (ie, respiratory support and antibiotics), nutrition and outcome (length of hospital stay and mortality).
Quality appraisal of included studies
Since the most common tools for assessing quality and/or risk of bias (such as Cochrane RoB tool, Risk of Bias in Non-Randomized Studies (ROBINS) and Metodological Index for Non-randomized Studies (MINORS)) are not adequate for observational studies such as case reports and case series, we used the tool proposed by Murad et al 14 for quality appraisal. The tool evaluates eight items under four domains (selection, ascertainment, causality and reporting) and can be applied to both case reports and case series.
The domain Selection includes one item that is graded as ‘high quality’ if the patient(s) represent(s) the whole experience of the investigator (centre) or ‘low quality’ if the selection method is unclear to the extent that other patients with similar presentation may not have been reported.
The domain Ascertainment includes two items (about exposure and outcome) that are graded as ‘high quality’ if exposure/outcome were adequately ascertained and ‘low quality’ otherwise. The items were graded ‘unclear’ if the ascertainment was not reported in a clear way.
The domain Causality includes an item on alternative causes (graded as ‘high quality’ if other alternative causes that may explain the observation were ruled out and ‘low quality’ otherwise) and an item on follow-up (graded as ‘high quality’ if the follow-up was long enough for outcomes to occur and ‘low quality’ otherwise). The items were graded ‘unclear’ if the ascertainment was not reported in a clear way. In this review, the other two items of Causality (about challenge/rechallenge phenomenon and dose–response effect) were not used because are mostly relevant to cases of adverse drug events.
The domain reporting includes one item that is graded as ‘high quality’ if the cases were described with sufficient details to allow other investigators to replicate the research or to allow practitioners make inferences related to their own practice and ‘low quality’ otherwise.
Two researchers (DT and FC) completed the quality appraisal by using the tool proposed by Murad et al, with a third researcher (EB) resolving any inconsistency.
Data synthesis
A narrative synthesis of included studies was conducted, because the study designs (case reports and case series) did not allow to perform a meaningful meta-analysis.
Results
Study selection
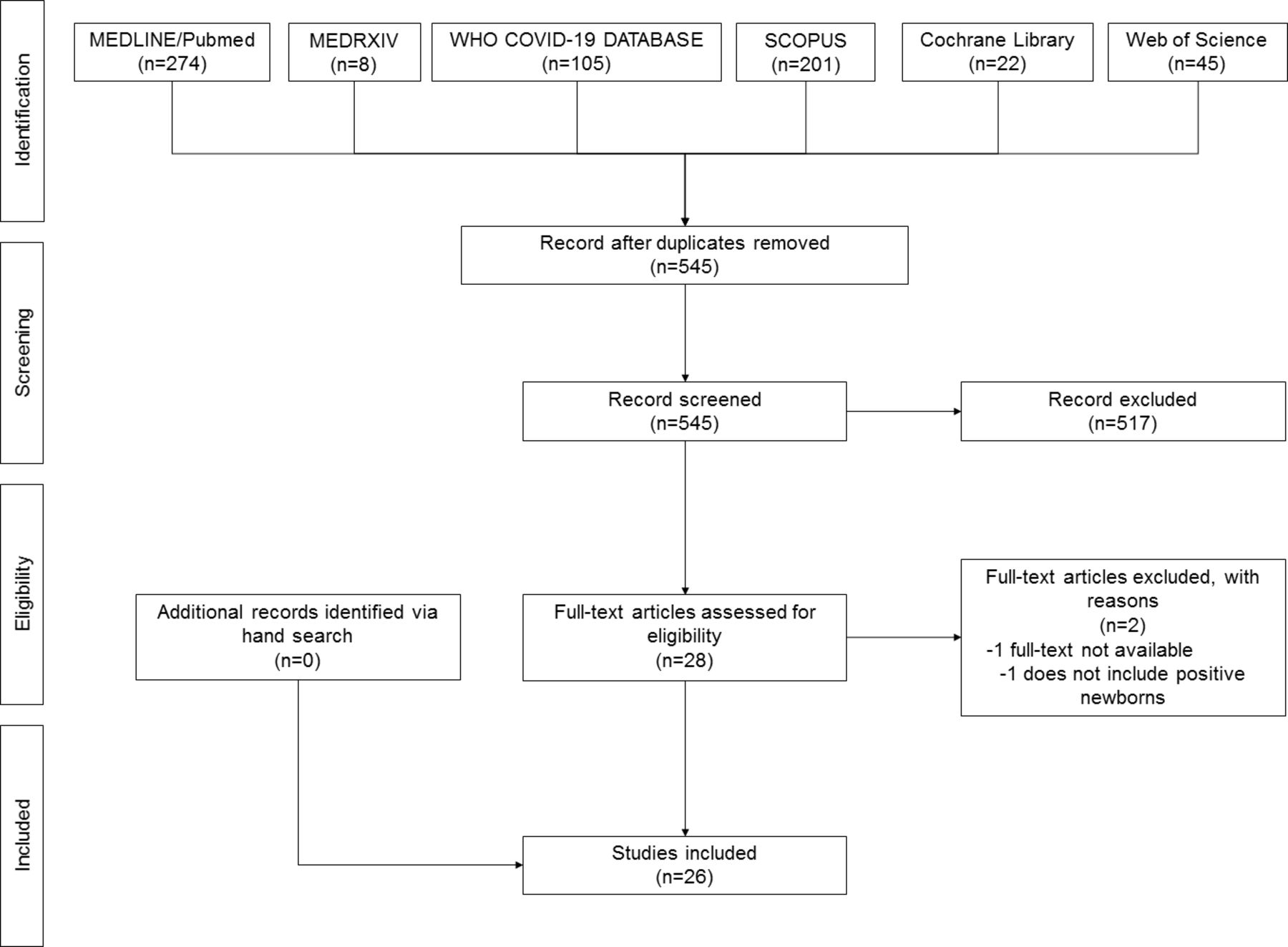
Overall, the searches yielded 545 non-duplicated articles. Of them, 517 articles were excluded after title and/or abstract screening, and 28 articles were retrieved for full-text review. Two studies were further excluded (one full-text was not available and one did not include positive neonates), and no additional studies were found via hand search. Ultimately, 26 observational studies (18 case reports and 8 case series) were included in the qualitative synthesis (figure 1).3 4 15–38 Twenty-four were in English and two in Chinese. Publication time was from March to May 2020. Main sources were China (10 studies) and Italy (five studies). A total of 44 newborns with SARS-CoV-2 infection were described (table 1).

Flow chart of included studies.
Summary of included studies
Quality assessment of included studies
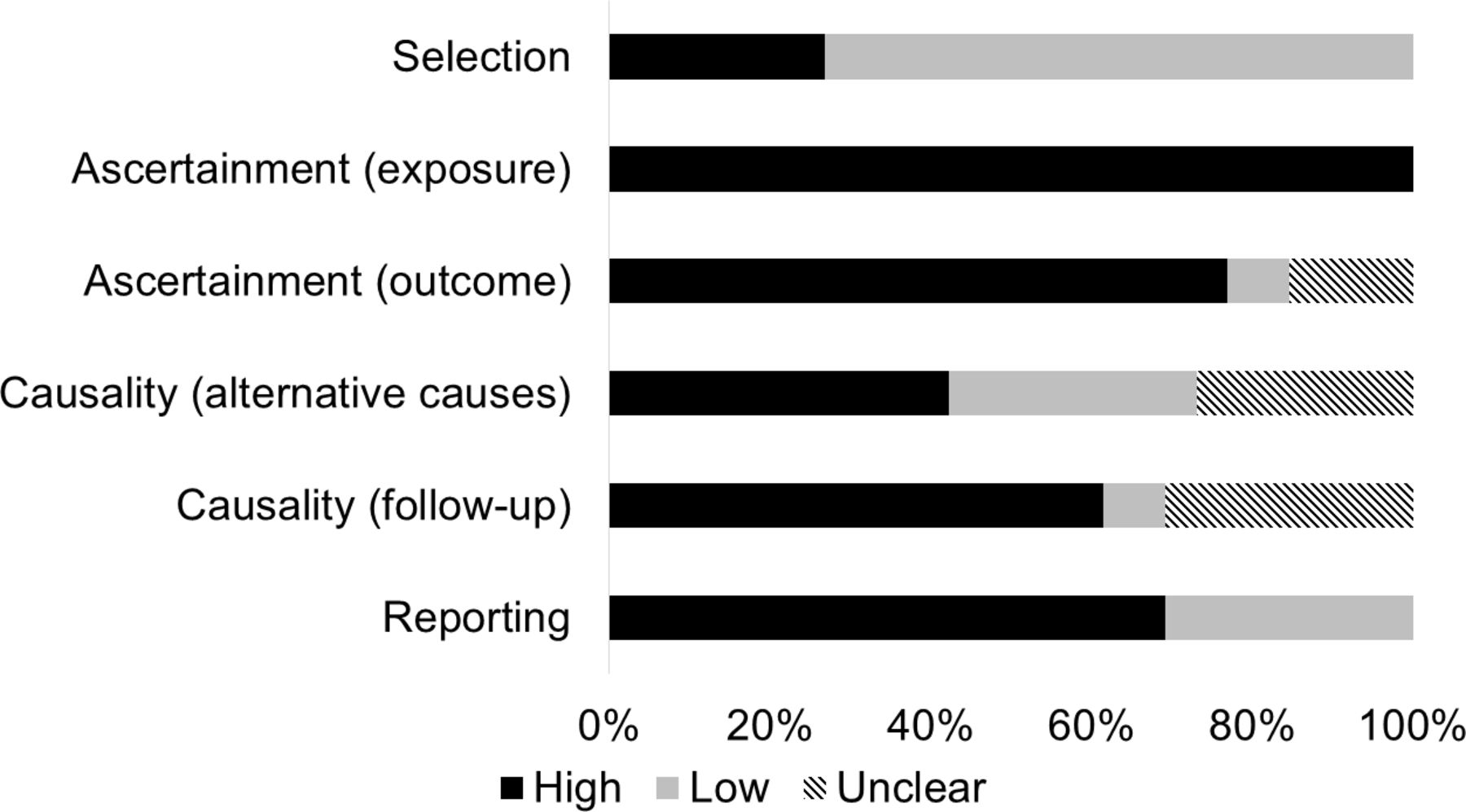
Summary of quality assessment is shown in figure 2. Quality of selection was high in seven studies (27%) where the patients represented the whole experience of the investigator/centre. All studies (100%) diagnosed SARS-CoV-2 infection using swab and/or serology (high quality of ascertainment of exposure), while 20 studies (77%) adequately ascertained the outcome measures (high quality). Other alternative causes (that may explain the observation) were ruled out in 11 studies (42%, high quality), and the follow-up was long enough for outcomes to occur in 16 studies (62%, high quality). Eighteen studies (69%) described the cases with sufficient details to allow other investigators to replicate the research or to allow practitioners make inferences related to their own practice (high quality). Details on quality assessment are reported in online supplemental table 1.
Supplemental material

{kind=link}
{kind=link}
Summary of quality assessment of included studies (case report and case series).
Demographics and diagnosis of neonates with SARS-CoV-2 infection
Demographics and diagnosis of neonates with SARS-CoV-2 infection are summarised in table 2. Diagnosis was achieved by swab in 41 neonates (median 1 positive swab, IQR 1–2) and by serology in three neonates. Among these, SARS-CoV-2 IgM and IgG concentrations were higher than normal level (<10 AU/mL) at day 1 (two neonates) and at days 2 and 16 (one neonate). Thirty-five mothers (80%) were tested positive for SARS-CoV-2 (31 by swab and 4 by swab+serology), and 32 of them were symptomatic. Contact with infected mother was reported in 16 neonates (44%). Median age at diagnosis was 5 days (IQR 2–17). Radiological pattern of pneumonia was indicated in 15/21 neonates (71%). Thirty neonates (68%) were admitted to neonatal ward immediately after birth, while 14 (32%) were admitted to hospital from home.
Summary of demographics and diagnosis of neonates with SARS-CoV-2 infection
Laboratory findings of neonates with SARS-CoV-2 infection
Few information about laboratory findings were reported in the included studies (online supplemental table 2). Abnormal white cell count was indicated in 3/21 neonates (14%), lymphopaenia in 4/17 (24%) and abnormal platelet count in 3/11 (27%). Alanine aminotransferase and aspartate aminotransferase were abnormal in 1/15 (7%) and 5/16 (31%) neonates. Positive blood culture was found in 2/13 (15%) neonates.
Supplemental material
Clinical characteristics, treatment and outcome of neonates with SARS-CoV-2 infection
Symptoms occurred in 26/38 neonates (68%) at median 10 days (IQR 2–19). The most common symptoms were fever (50%), gastrointestinal symptoms (26%), hypoxia (20%) and cough (20%). The majority of neonates (27/36, 75%) were managed in spontaneous breathing (room air). Nutrition with formula was used in 17/28 neonates (61%). All neonates were discharged at a median length of hospital stay of 10 days (IQR 6–14) (table 3).
Clinical characteristics, treatment and outcome of neonates with SARS-CoV-2 infection
Discussion
This review offers an overview of published cases of neonates with SARS-CoV-2 infection during the 2019–2020 pandemic. To date, 26 studies (case reports and case series) described a total of 44 infected neonates.
To our knowledge, this is the first systematic review focusing on neonates with confirmed SARS-CoV-2 infection. Clinical data from infected adults and children have been available since January and February 2020, respectively, while information on infected neonates has become available since March 2020.10 Although SARS-CoV-2 infection is still spreading worldwide, this review on the first published cases can provide useful information to help clinicians and stakeholders in the management of neonates with SARS-CoV-2 infection.
Overall, SARS-CoV-2 infection was diagnosed with a swab (nasopharyngeal, throat or anal) in all neonates but three at median 5 days of life. The source of infection in neonates remains unclear. Around half of neonates had a documented contact with the infected mother, thus suggesting contact with different infected subjects (ie, family members or health caregivers) for the other neonates. Of note, one out of three infected neonates was admitted from home. Vertical (intrauterine) transmission of SARS-CoV-2 has been hypothesised39 but is difficult to rule out.3 4 40 In addition, respiratory viruses (ie, Middle East respiratory syndrome coronavirus and SARS) did not show infection through vertical (intrauterine) transmission.39
It is noteworthy that about a quarter of infected neonates were asymptomatic, while the majority showed mild symptoms typical of acute respiratory infections (such as fever, hypoxia and cough), in agreement with available data on children.10 11 Neonates were more like to present with gastrointestinal symptoms (26%) compared with literature information on children and adults.11
Respiratory management was performed according to the mild clinical status of infected neonates, with the majority of them left in spontaneous breathing (room air). Only 1 out of 10 neonates needed mechanical ventilation, but we cannot exclude that concomitant conditions (ie, prematurity) may have contributed to the clinical status.
Nutrition of neonates during SARS-CoV-2 pandemic requires specific considerations.41 42 Breast feeding from infected mothers remains a conflicting aspect, with some institutions supporting breast feeding under appropriate precautions43–45 and other institutions recommending milk formula.46 Breast milk samples from six infected mothers were tested negative for SARS-CoV-2 by Chen et al,40 but more information is needed to rule out this route of transmission. Our findings mirror such heterogeneous positions, with 28% of neonates receiving breast feeding, 11% feeding on maternal milk but not in contact with the mother and 61% not feeding on maternal milk and not in contact with the mother.
Overall, prognosis of neonates with SARS-CoV-2 infection was good, with all of them discharged alive after a median hospital stay of 10 days. While median duration of hospitalisation was comparable among neonates, children and adults,11 47 48 literature data stress the different impact of the disease in neonates/children versus adults who have worse prognosis.7 Many hypotheses have been suggested to explain this fact, including a lower ACE2 expression, the receptor that SARS-CoV-2 uses for host entry, less proinflammatory cytokine response, a stronger innate immune response and a higher proportion of total lymphocytes and absolute numbers of T and B cells.49 50 Of note, recent literature suggested some differences in prognosis within paediatric population, where being younger than 1 month was associated with increased likelihood of admission to intensive care unit.51 Furthermore, children may require less intensive care support than adults, but each child is expected to occupy the intensive care bed for prolonged time, with relevant consequences on service planning.51
Our findings should be interpreted within some limitations. First, all included studies were case reports and small case series, with low quality of reporting and generalisability. Second, the pandemic is not concluded yet, thus this review offers only preliminary findings, as more cases are expected to be reported in the next future. However, the summary of available literature can guide health caregivers in the management of neonates infected with this new virus, as well as suggest areas of improving for future reporting.
Conclusions
This systematic review summarises clinical data and management of neonates with SARS-CoV-2 infection. All evidence results from case reports and small case series, mainly from China and Italy. Source of infection remains unclear because around half of neonates had a documented contact with the infected mother, and one out of three infected neonates was admitted from home. One out of four neonates was asymptomatic, and the remaining showed mild symptoms typical of acute respiratory infections and/or gastrointestinal symptoms. The majority of neonates were left in spontaneous breathing (room air) and had good prognosis after a median duration of hospitalisation of 10 days. Nutrition policy was heterogeneous (including breast feeding, pump milk and formula), mirroring the different international recommendations. While this review offers a preliminary overview of clinical data and management of neonates with SARS-CoV-2 infection, large epidemiological and clinical cohort studies, as well as the implementation of collaborative networks, are needed to improve the understanding of the impact of SARS-CoV-2 infection in neonates.
Data availability statement
Data are available on reasonable request.
References
Footnotes
DT and FC contributed equally.
Contributors DT conceived and designed the study, contributed to draft the manuscript and approved the final manuscript as submitted. FC analysed the data, contributed to draft the manuscript and interpret the results and approved the final manuscript as submitted. MEC reviewed search results and screened titles/abstracts, extracted key data from the included studies, contributed to draft the manuscript and approved the final manuscript as submitted. MB conducted the literature search, reviewed search results and screened titles/abstracts, contributed to interpret the results, critically revised the manuscript and approved the final manuscript as submitted. SC extracted key data from the included studies, contributed to interpret the results, critically revised the manuscript and approved the final manuscript as submitted. EB conceived and designed the study, critically revised the manuscript and approved the final manuscript as submitted. All authors are responsible for the accuracy and the integrity of the data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.