Article Text

Abstract
Background Periorbital necrotising fasciitis (PNF) is a devastating infection of subcutaneous soft tissue and underlying fascia causing severe morbidity and even loss of life. Few case reports of PNF exist and there are no prospective epidemiological studies.
Methods A prospective observational study was undertaken using the British Ophthalmological Surveillance Unit reporting system. Questionnaires were sent to reporting ophthalmologists in the UK seeking cases of PNF over a 2-year period.
Results 30 new cases were confirmed. 16 of the reported cases followed a precipitating event, 9 cases followed trauma and 3 followed surgery. β-haemolytic Streptococcus A was the causative organism identified in 76%, either alone or with concurrent infection, and antibiotic sensitivities are discussed. Systemic complications occurred in the majority of cases (66.6%), with sepsis and death occurring in 10%. Over 50% of surviving patients had subsequent morbidity, reduced acuity (<6/18) being common.
Conclusion PNF is a rare, dangerous condition. This study identified an incidence of 0.24 per 1 000 000 per annum in the UK. β-haemolytic Streptococcus A is the most common causative organism. Mortality remains a potential outcome, and survivors suffer significant morbidity. Early intravenous antibiotic management with a consensus favouring penicillin and clindamycin combined with debridement.
- Epidemiology
- Eye Lids
- Orbit
- Infection
- Pathology
Statistics from Altmetric.com
Introduction
Necrotising fasciitis is a potentially lethal infection of subcutaneous tissue and underlying fascia arising from the angiothrombotic microbial invasion and liquefactive necrosis of soft tissues.1 Bacteria release collagenase and hyaluronidase, contributing to aggressive tissue destruction. Polymorphonuclear leucocytes infiltrate deep tissues, and blood vessels passing through fascia thrombose. Tissue invasion proceeds horizontally due to the avascularity of fascial planes. As the condition progresses, ischaemic necrosis of the skin, subcutaneous fat and dermis develops.2–4
Patients present with signs of cellulitis and disproportionate pain. As the condition progresses, tissues become increasingly erythematous and oedematous before breaking down. Very quickly patients become systemically unwell. The Laboratory Risk Indicator for Necrotising Fasciitis may assist diagnosis5 and leucocytosis has been shown to have a 90% sensitivity and specificity.6
Rarely, necrotising fasciitis affects the periorbital region. Outcomes range from disfigurement and sight loss, through to death. A review by Lazzeri et al7 identified 104 published reports of periorbital necrotising fasciitis (PNF) between 1950 and 2008. A 2012 review by Amrith et al6 traced 94 cases in the past 20 years. To our knowledge, no large prospective epidemiological studies have been conducted for PNF.
Methods
Prospective case ascertainment was undertaken using population-based active surveillance through the British Ophthalmological Surveillance Unit (BOSU).8 Using a monthly report card, all UK consultant and associate specialist ophthalmologists were asked to report new cases of periorbital fasciitis identified between April 2010 and April 2012.
Reporting ophthalmologists were sent an incident questionnaire and a 6 month review questionnaire. These sought information including demographics, precipitating events, microbiology, antibiotic sensitivity, morbidity and mortality, and visual outcomes.
Results
Forty potential cases of PNF were reported. Thirty questionnaires were completed and returned with confirmation of the diagnosis; three were reported not to be PNF following an initial incorrect diagnosis. There was no response for the remaining seven cases. Ultimately, complete data was obtained for 30 new cases of PNF over a 2-year period in the UK.
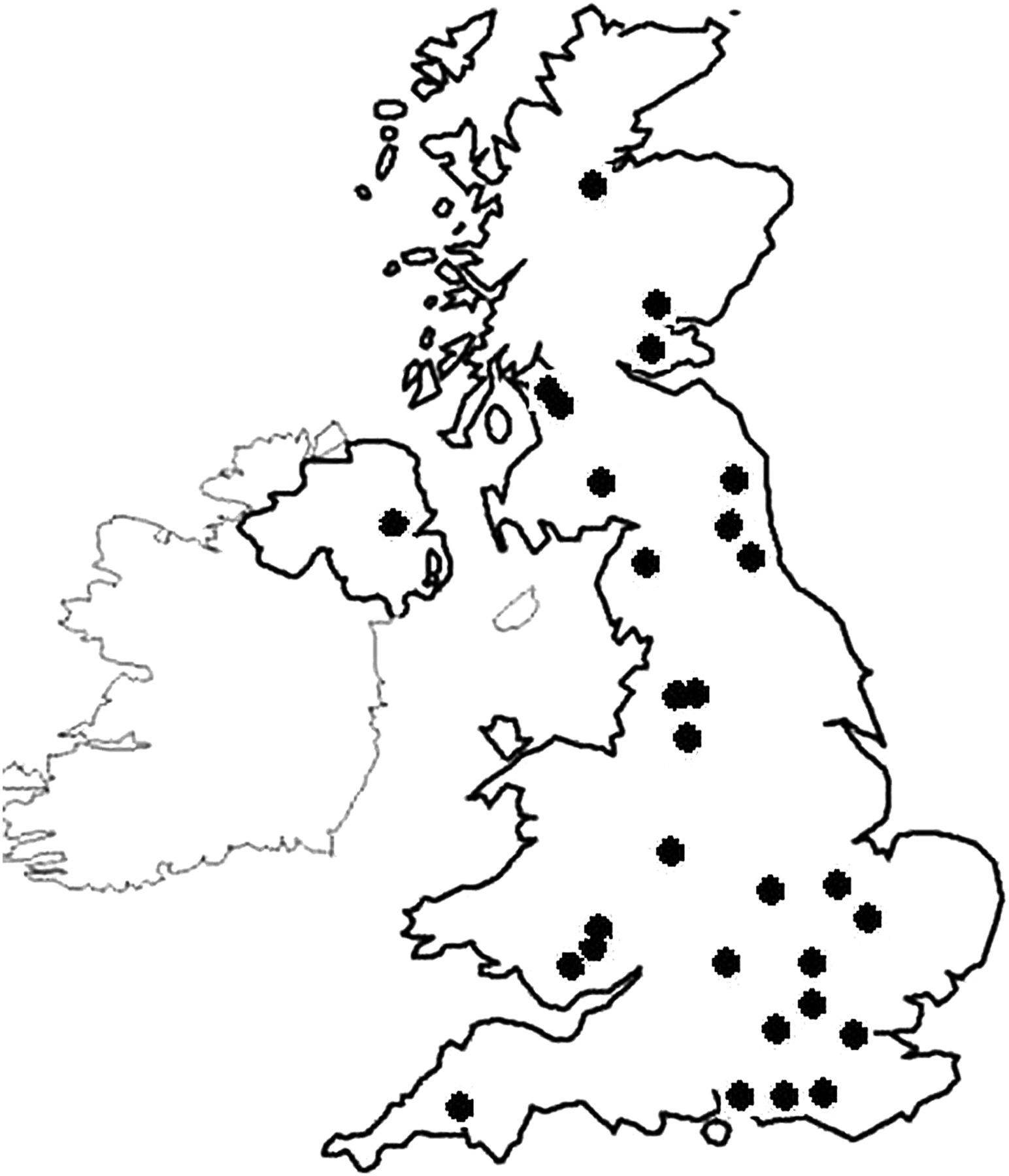
Cases were reported from around the UK (figure 1). Patients ranged in age from 33 years to 88 years, with a median age of 68 years. Seventeen women were affected, and 13 men. Laterality was evenly distributed; 10 left eyes were affected alone, 10 right eyes were affected alone, and 10 cases had bilateral involvement.

Thirty cases of periorbital necrotising fasciitis were identified across the UK.
Risk factors
Rarely was there predisposing ophthalmic history. (One patient had a corneoscleral abscess). Patient medical history included several conditions impacting the immune system that may have contributed to PNF development; two patients were on lymphoma chemotherapy, one patient had diabetes, one patient had endometrial cancer,9 one patient had prostate cancer,9 two patients were alcoholic, one had end-stage renal failure, one patient had thyroid disease, and four patients were on long-term steroids—one for rheumatoid arthritis, two for chronic obstructive pulmonary disease (COPD) and one for polymyalgia rheumatica.
Triggers
Potential precipitating events were identified in 16 cases; 9 patients had trauma to the area, 3 had recent surgery on nearby areas (1 blepharoplasty, 1 temple basal cell carcinoma (BCC) excision, 1 ethmoidal artery ligation with cantholysis), 2 patients presented with primary pharyngitis, another with conjunctivitis, and 1 with a ‘forehead lump’ days before developing PNF symptoms.
Multidisciplinary management
Ophthalmology was involved in managing every case. Contributing specialties included infectious diseases, maxillofacial surgery, ear, nose and throat (ENT), intensive treatment unit (ITU), high dependency unit (HDU), rheumatology and general medicine. There was little delay in ophthalmology review. Ten patients were seen within 24 h of the onset of symptoms, 11 more within 48 h, and only 6 waited longer. (On three occasions the time until ophthalmology review was not reported). Management preceding ophthalmology review included various broad-spectrum antibiotics; one patient had surgical debridement by a maxillofacial surgeon.
Visual outcomes
Formal visual acuity was obtained at presentation for 22 affected eyes. Of these, 10 were less than 6/60. Following treatment, this generally improved. However, at 6 months, 2 eyes had no perception of light, and 9 of the 26 eyes with a follow-up assessment had a visual acuity of 6/18 or worse (figure 2). Only one case with a final acuity of less than 6/18 had pre-existing eye disease (dry macular degeneration.)
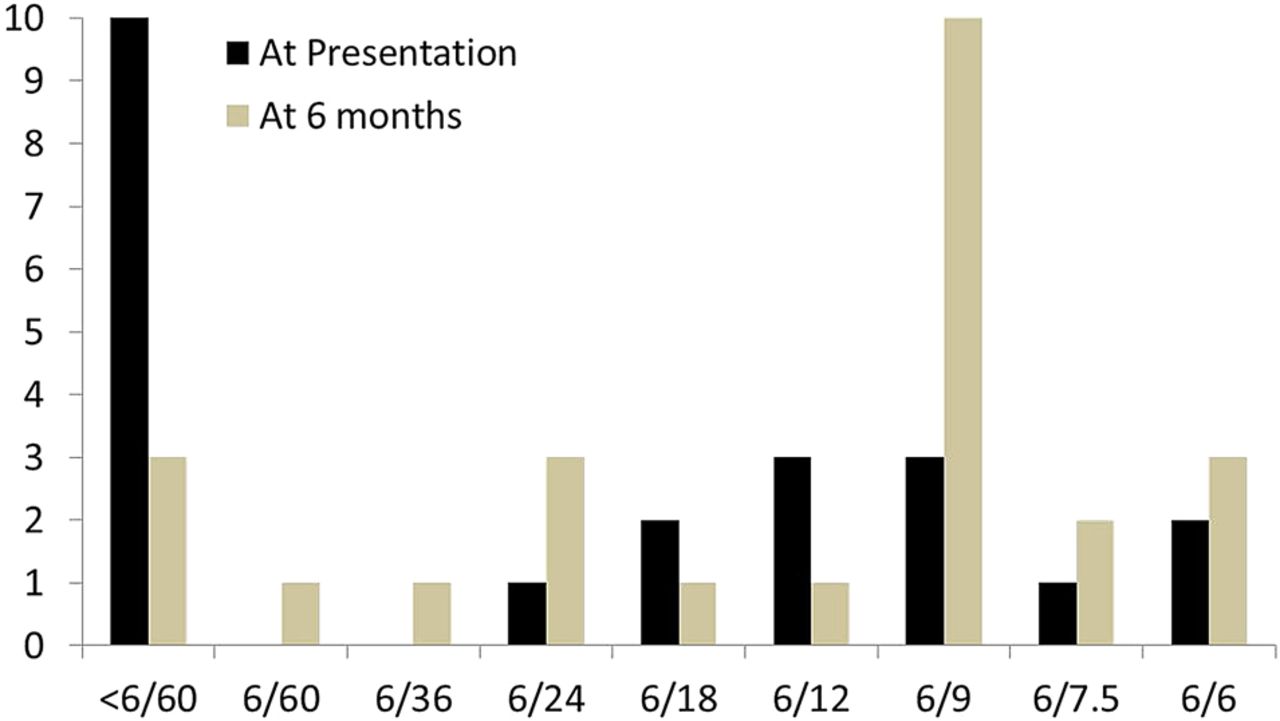
Number of patients achieving a given visual acuity at presentation and at 6 months.
Eyelid cellulitis and necrosis
Patients with the least eyelid necrosis had the least residual morbidity (figure 3). The converse was also true: eyes with a final visual acuity of 6/18 or worse had upper and lower eyelid cellulitis and at least one eyelid affected by necrosis. The five eyes with a final acuity less than 6/36 had medial upper eyelid necrosis and orbital involvement. The only patient requiring exenteration had loss of more than 50% of the upper and lower eyelids.

Frequency of cellulitis (and necrosis) in affected lids by area.
Two patients who died had bilateral cellulitis and necrosis; one affecting upper and lower eyelids, one with only upper eyelid involvement. The third deceased patient had bilateral cellulitis and monocular necrosis affecting the upper and lower eyelids.
Facial involvement
Extension to surrounding dermatomes was recorded. In 23 eyes (57.5%), significant spread affecting the V1 dermatome was reported. In 17 eyes (42.5%), this spread to V2, and in 8 eyes (20%), spread encompassed V1–V3. No cervical or mediastinal involvement was reported.
Orbital involvement
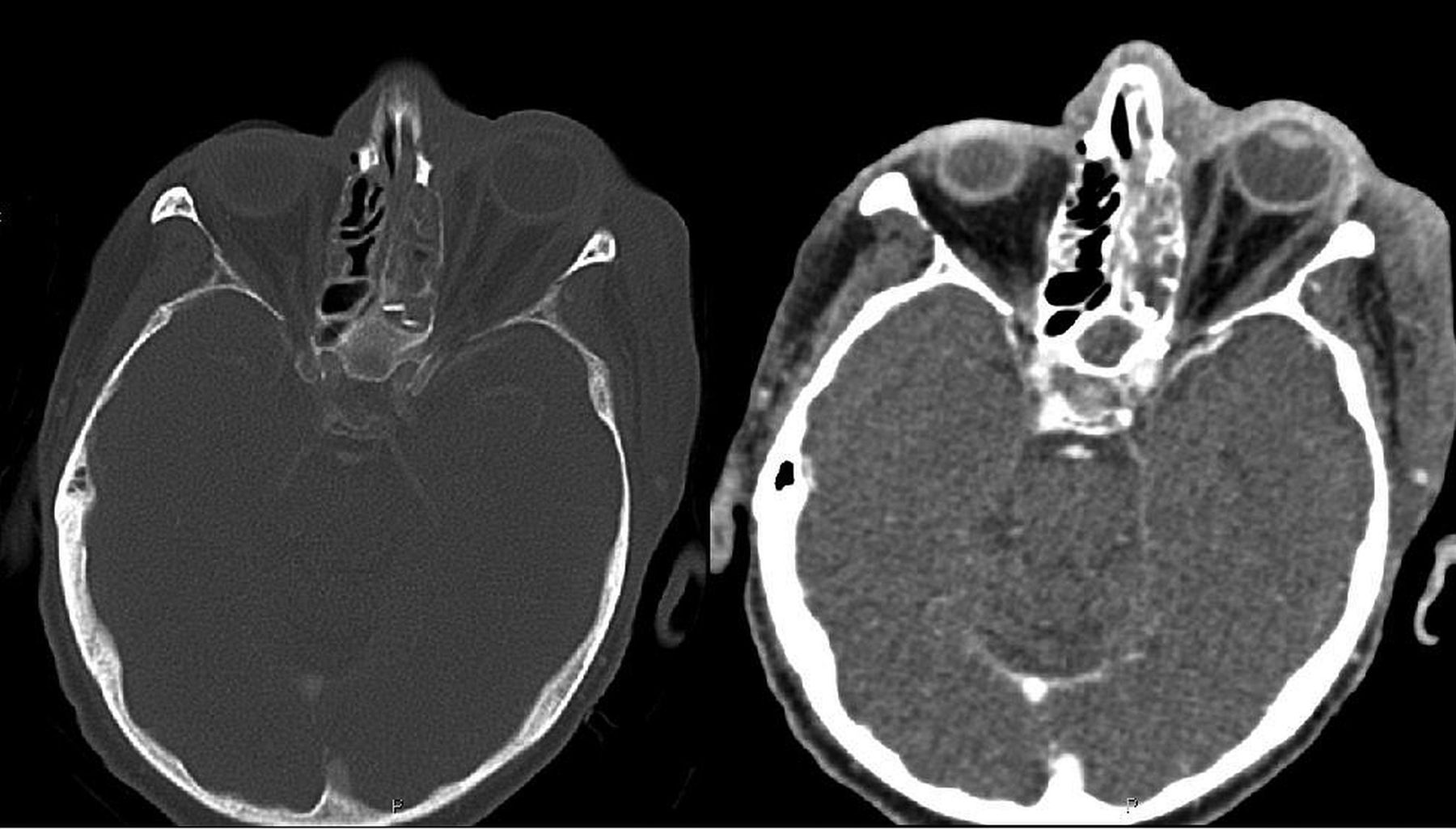
Clinically, orbital involvement (infection behind the orbital septum,) presented as motility problems in 12 eyes, proptosis in 8 eyes and relative afferent pupillary defect (RAPD) in 9 eyes. One patient reported pain on eye movements. All patients had CT imaging (figure 4).

CT showing facial soft tissue and orbital involvement with proptosis.
Necrosis affecting the medial upper lid was the only outward sign common to all patients with orbital involvement. (Medial upper lid necrosis did not always indicate orbital involvement.)
Orbital involvement was the biggest predictor of poor visual outcome (all five eyes with a final visual acuity of 6/36 or less had orbital involvement) and the only patient requiring exenteration had orbital involvement. None of the patients who died had orbital involvement.
Systemic involvement
Three patients suffered renal failure, and five patients developed toxic sepsis; one patient with sepsis progressed to disseminated intravascular coagulation. One patient had pulmonary emboli, and another developed pneumonia.
Causative organism
Group A β-haemolytic streptococcus was cultured in the vast majority of cases, (22 out of 29 successful cultures, or 76%.) In 18 cases, it was the sole organism; in four cases, it was a co-infection. Pseudomonas was cultured as the sole organism in two cases, and in one case as a co-infection. Staphylococcus aureus was cultured in four cases, but only ever as a co-infection.
Management
Treatment with intravenous antibiotics was universal and a wide variety of intravenous antibiotic combinations were used. Intravenous penicillin with clindamycin was the most common first line combination prescribed by ophthalmologists. It was not possible to identify any one combination that was singularly effective (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Antimicrobial therapy prescribed to treat periorbital necrotising fasciitis. IV, intravenous.
Twenty-one patients had surgical debridement within 10 days of diagnosis. Mean time to surgery is not known. The nine patients who did not have surgical debridement had comparable vision and morbidity outcomes to those that did.
A single patient required exenteration. Fifteen patients required reconstructive surgery for tissue loss. Procedures included skin grafts, conjunctival flaps for corneal perforation, ptosis correction, entropion correction, tarsorrhaphy and scar release. Patients requiring surgery usually had one procedure, but one patient required three procedures and one patient had four procedures. The patient who had exenteration had a total of eight procedures.
Hyperbaric therapy has been described as a treatment adjunct for necrotising fasciitis but was not used by the treatment centres in our study.10
Morbidity
Premorbid conditions offered no indication of final morbidity. Necrosis of any part of an eyelid was the single biggest indicator for surgery.
Ten patients were discharged before the study ended, 1 was lost to follow-up and 12 were still receiving treatment. At the time of the last questionnaire, 2 patients were awaiting surgical procedures and 11 were receiving lubricants for dry eyes.
Mortality
Three patients (10%) died due to multiorgan failure arising from PNF. One was initially misdiagnosed at an emergency department with 2 days delay before treatment, one patient spent several months on ITU and HDU with sepsis before dying, and one patient died within 5 days from toxic shock, renal failure and cardiac arrest.
One patient who died had COPD, one had pre-existing renal failure and one had no significant medical history.
Two patients who died had bilateral necrosis; one had upper and lower lid involvement, while one had only upper lid involvement. The third deceased patient had unilateral upper and lower lid necrosis with extensive facial spread.
One patient had β-haemolytic streptococcus A infection, and one patient had a mixed growth of β-haemolytic streptococcus A and staphylococcus aureus. One patient had no identified causative organism.
All three patients who died had intravenous antibiotics, including the consensus combination of clindamycin and penicillin.
Discussion
PNF is a rare condition with rates of morbidity and mortality. This study identified an incidence of 0.24 per million per annum. This number is based on a mid-study UK population of 63 million people as identified by the Office of National Statistics.
We worked to minimise underascertainment by using a methodology proven effective.8 ,11 ,12 We report minimum incidence as under-reporting of a rare condition is likely. To our knowledge, no large prospective studies exist and this study therefore provides important incidence data. The return rate of the BOSU system for our study was 77% indicating high compliance. Studies using this methodology previously reported ascertainment rates between 69% and 100%.8 Although it is likely that a proportion of the seven cases for which no information was collected are not true cases, if they were to be included and assuming an ascertainment rate of 69%, the incidence could be higher. It may therefore lie between 0.24 and 0.45 per million per annum.
Predictably, trauma was a common predisposing factor; surgery to a lesser extent. Many cases had no identifiable trigger. Understandably, immune suppression was a frequent risk factor, being present in more than a third of cases. However, this data is at odds with a recent review article stating that type 1 infections in the periorbital area are not associated with immunocompromised status.6
β-haemolytic Strep A was the most common causative organism, cultured in 76% of cases. This concurs with other studies, reporting incidence from 50% to 70%.6 ,7 ,13–15 It was the causative organism in two of the three deaths. (No culture was obtained for the third patient.) Decisions regarding early management should consider this.
Intravenous antibiotic treatment was universal. Following ophthalmology review, the consensus strategy was a penicillin with clindamycin at presentation, escalating to higher generation penicillins and atypical antibiotics as required. Antibiotic combination was widespread with no consensus beyond the initial combination of clindamycin with penicillin.
The majority of cases identified by Lazzeri et al7 and Amrith et al6 involved surgical management. There are, however, advocates of conservative management. Luksich et al16 published a case series of seven patients with PNF restricted to the eyelids treated successfully with medical management alone. The nine cases in this study managed without surgery had similar outcomes to patients undergoing debridement. The fact that 9 out of 30 cases were managed non-surgically was a surprise to the authors. There is no bias towards conservative management among the authors and we believe that shrewd clinical judgement is required, with a low tolerance to proceed to theatre when sight or life is threatened.
Reduced vision following PNF was common. Vision generally improved from initial presentation, but reduction to 6/18 or worse occurred in a third of patients. Orbital involvement was the single biggest risk factor for poor visual outcome, being present in both patients with a no perception of light (NPL) visual outcome and all five patients with a final acuity of 6/36 or less.
Summary
In summary, PNF is a rare dangerous condition, with an incidence of 0.24 per million per annum. It affects people of all ages, often following trauma or surgery and often in those with immune suppression. It has a mortality rate of 10%, and residual morbidity is frequent; dry eye symptoms, and reduced visual acuity (<6/18 in 30%) being commonplace. Early diagnosis, aggressive antibiotic management, most commonly with penicillin and clindamycin, coupled with surgical debridement, are the cornerstones to successful outcomes. Empirical treatment decisions should bear in mind β-haemolytic Streptococcus A is the causative organism in over 75% of cases, but that it is not the only causative organism.
Acknowledgments
The authors thank Dr Umiya Agraval for presenting on behalf of their group at the Oxford Ophthalmological Congress 2013.
References
Footnotes
-
Contributors PWF contributed to the acquisition, analysis and interpretation of the data for the work, drafted the manuscript and revised it for publication. PC contributed to the conception of the idea and reviewed the work prior to submission. MEG contributed to the acquisition of data from reporting consultants. BF contributed to the design of the research and to the analysis of the data. He also wrote a paragraph of the manuscript. SRD contributed to the conception of the idea, obtained ethics approval and wrote the questionnaires for the research. She also was the main reviewer of the manuscript prior to submission.
-
Competing interests None.
-
Ethics approval Ethics approval came from the West of Scotland Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.