Article Text

Abstract
The posterior reversible encephalopathy syndrome is an increasingly recognised disorder. Most patients have several symptoms; seizures are the most frequent, often multiple or status epilepticus. A combination of seizures, visual disturbance and/or headache, in particular, should lead to an early brain MRI to reveal the typical pattern of bilateral hyperintensities on fluid attenuated inversion recovery imaging, predominantly in the parieto-occipital region. There seem to be many possible triggers, including abrupt arterial hypertension, impaired renal function, pregnancy, immunosuppressive therapies and various inflammatory conditions. The clinical outcome is excellent, with recovery within a few days, while the MRI abnormalities resolve much more slowly. Little is known about the best management. Seizures do not normally progress to chronic epilepsy so antiepileptic drugs should be discontinued after about 3 months.
Statistics from Altmetric.com
Introduction
What is now known as the posterior reversible encephalopathy syndrome (PRES) was first described as posterior reversible leukoencephalopathy by Hinchey and colleagues1 in 1996. The major symptoms were headache, vomiting, confusion, seizures and visual abnormalities in combination with a typical imaging pattern of bilateral white matter abnormalities in the posterior regions of both cerebral hemispheres. Since then, PRES has attracted increasing interest and there have been many publications, mostly case reports and imaging studies. Only a few publications have been concerned with the clinical features.
PRES is sporadic and its incidence is unknown but it has been reported worldwide without any gender differences.2 3 Both children and older people can be affected.4
There has been much discussion about the proper name for this syndrome because the posterior brain region is not always affected, the cortex can be involved and there have been cases with irreversible lesions. The most common name is PRES. ‘PRES’ is easy to pronounce and reminds one of the word (blood) pressure which is postulated to be one of the most common trigger factors.5
In this review we will discuss what we know and what is new about the clinical and imaging features of the syndrome, the differential diagnosis, possible pathogenic mechanisms, prognosis (without and with treatment) and management.
Clinical picture
Although PRES can be a severe neurological disease, recovery is the rule. However, it does have a differential diagnosis which includes many life threatening disorders such as posterior circulation ischaemic stroke. The apparent severity at early presentation can lead to unnecessary diagnostic procedures such as cerebral angiography or lumbar puncture. Moreover, because the clinical findings are not specific, these patients are often treated on intensive care units before the correct diagnosis is made; in fact, intubation and mechanical ventilation are very rarely necessary.6
PRES is a syndrome with visual loss, headache, altered mental function, seizures and nausea. There are seldom any prodromal symptoms such as exhaustion, tiredness or aches and pains. The symptoms usually develop quite quickly over a few hours, reaching their worst in 12–48 h. Progression over several days is uncommon, and the symptoms usually resolve within a week but may persist for longer in a few cases. Most authors have emphasised the visual loss and headache. But, if one takes a closer look at the frequency of the symptoms, it becomes obvious that seizures are the most frequent, in up to 90% of cases and often preceding any of the other manifestations.3 7 8 This may well present a diagnostic problem because seizures disorders are so common in patients who are admitted via an emergency department, brain CT only shows lesions in PRES in about 50% of cases (see below), and brain MRI is not always performed—hence the diagnosis can easily be overlooked unless other symptoms are recognised. Isolated symptoms in PRES, such as seizures, are in fact rare which should provide a diagnostic clue that one is dealing not with ‘just epilepsy’, and so lead on to an early brain MRI, not being content with the false reassurance of a ‘normal CT scan’.
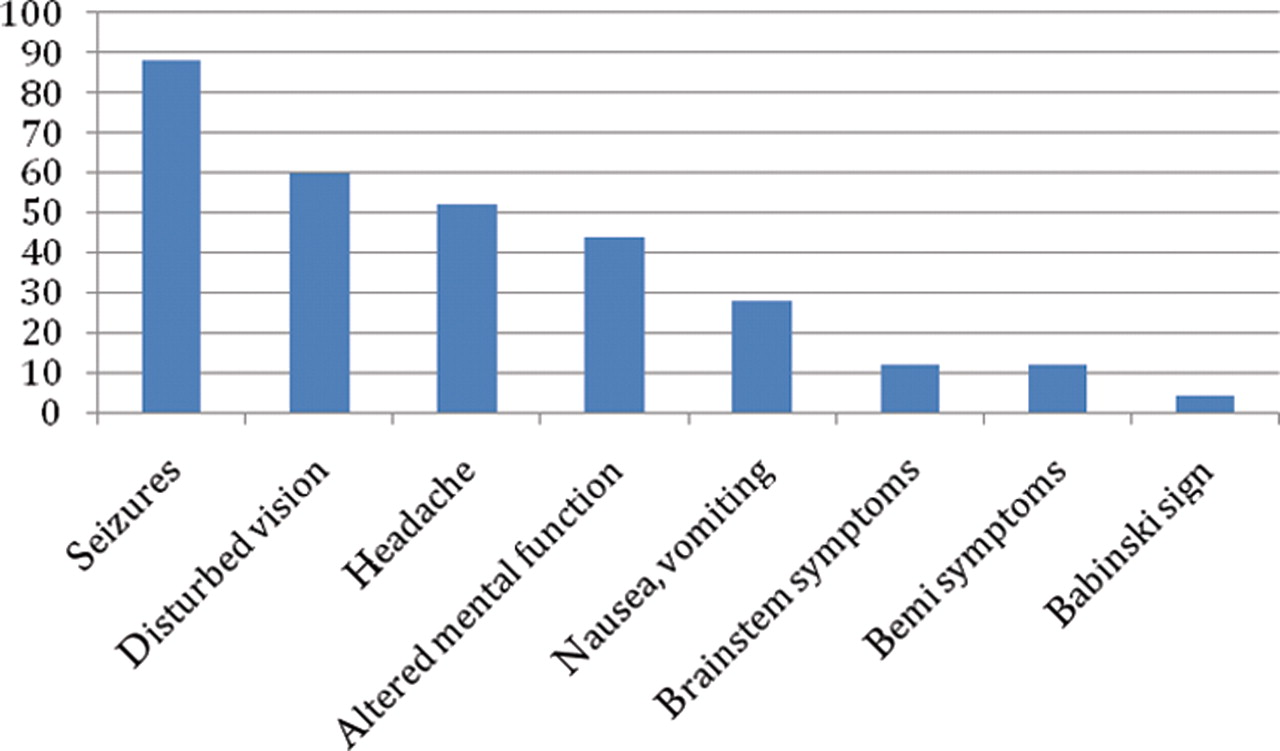
Analysing the number of symptoms per patient in our own PRES cohort of 33 patients, only two had seizures without any other symptom. Most had three or four different symptoms (figure 1). As well as seizures, the most common symptoms were disturbed vision, headache and altered mental function. We have never seen patients with isolated minor symptoms such as nausea or hemiparesis. A combination of seizures with disturbed vision and/or headache, in particular, should lead to an early MRI.

Frequency (%) of posterior reversible encephalopathy syndrome signs and symptoms.5
Seizures are generalised tonic–clonic but may start focally. A sequence of generalised seizures is common, and status epilepticus may occur. Kozak and colleagues9 described 10 patients with status epilepticus as the initial manifestation in a cohort of 77 PRES patients (13%). Eight of these 10 patients in fact had non-convulsive status epilepticus with subtle clinical signs such as eye blinking or automatisms. In all cases, complete resolution of seizures was achieved with a combination of antiepileptic drugs. Seven of the 10 received only short term medication, at the most for 4 months, without any recurrent seizures.9 However, because altered mental function is a frequent symptom in PRES, diagnosing non-convulsive status epilepticus may be difficult and so we use EEG monitoring in all suspected PRES patients with altered mental function to detect subtle electrographic seizures.10
Disturbed vision is a frequent symptom due to the involvement of the occipital lobe; not only cortical blindness or homonymous hemianopia but also blurred vision, visual neglect and visual hallucinations. The fundus examination and pupillary responses are usually normal.
Altered mental function is very frequent. This may conceal other symptoms such as disturbed vision and nausea. Patients can be confused, lethargic with slowed motor responses or deeply stuporose. It is sometimes difficult to differentiate this state from a prolonged postictal period but our general impression is that altered mental function in PRES persists for several days, whereas postictal confusion improves within hours.
Headache is usually bilateral and dull in nature.
Other neurological features. Nausea and vomiting occur less frequently. Tendon reflexes are often brisk but symmetrical. Hemiparesis, Babinski's sign and brainstem features may occur occasionally.
Blood pressure. Because acutely raised blood pressure is found in most PRES patients,1,–,3 8 it has been thought to be an important aetiological factor. The mean peak systolic blood pressure ranges between 170 and 190 mm Hg.1 3 8 On the other hand, there are patients with normal blood pressure who have developed PRES. Perhaps, therefore, the raised blood pressure is required to sustain cerebral blood flow and is reactive rather than a cause of PRES. As of now, there is no study which has shown that blood pressure is raised before the onset of PRES.
A combination of seizures with disturbed vision and/or headache, in particular, should lead to an early MRI
Imaging
CT is generally the first investigation for patients with acute neurological disorders. Unfortunately, CT scans in PRES show lesions in only about 50%.8 Usually both occipital lobes are involved. The lesions are of low density which may lead to confusion with the top of the basilar artery syndrome and occipital infarction. But a typical PRES pattern mostly spares the paramedian occipital structures below the sulcus calcarinus while posterior lobe infarction is restricted to the territory of the posterior cerebral arteries.
MRI is the gold standard and should be performed as soon as PRES is suspected. The lesions are bright on T2 weighted and fluid attenuated inversion recovery (FLAIR) imaging. FLAIR, with nulling of the CSF, is more sensitive than T2 weighted MRI alone, all the more so for small subcortical and especially for cortical lesions. In a study of 16 PRES patients, subtle lesions were undetectable in four patients on MRI using just T2 weighted imaging without FLAIR.5 Although PRES is often thought to be a leukoencephalopathy, the cortex and deep gray mater can be seen to be involved on FLAIR in up to 94% of cases.5 Patients with extensive lesions on T2 weighted imaging tend to have a worse prognosis.11 Typical PRES lesions on MRI represent vasogenic oedema which can be distinguished by diffusion weighted imaging (DWI) (see below).
MRI is the gold standard and should be performed as soon as PRES is suspected
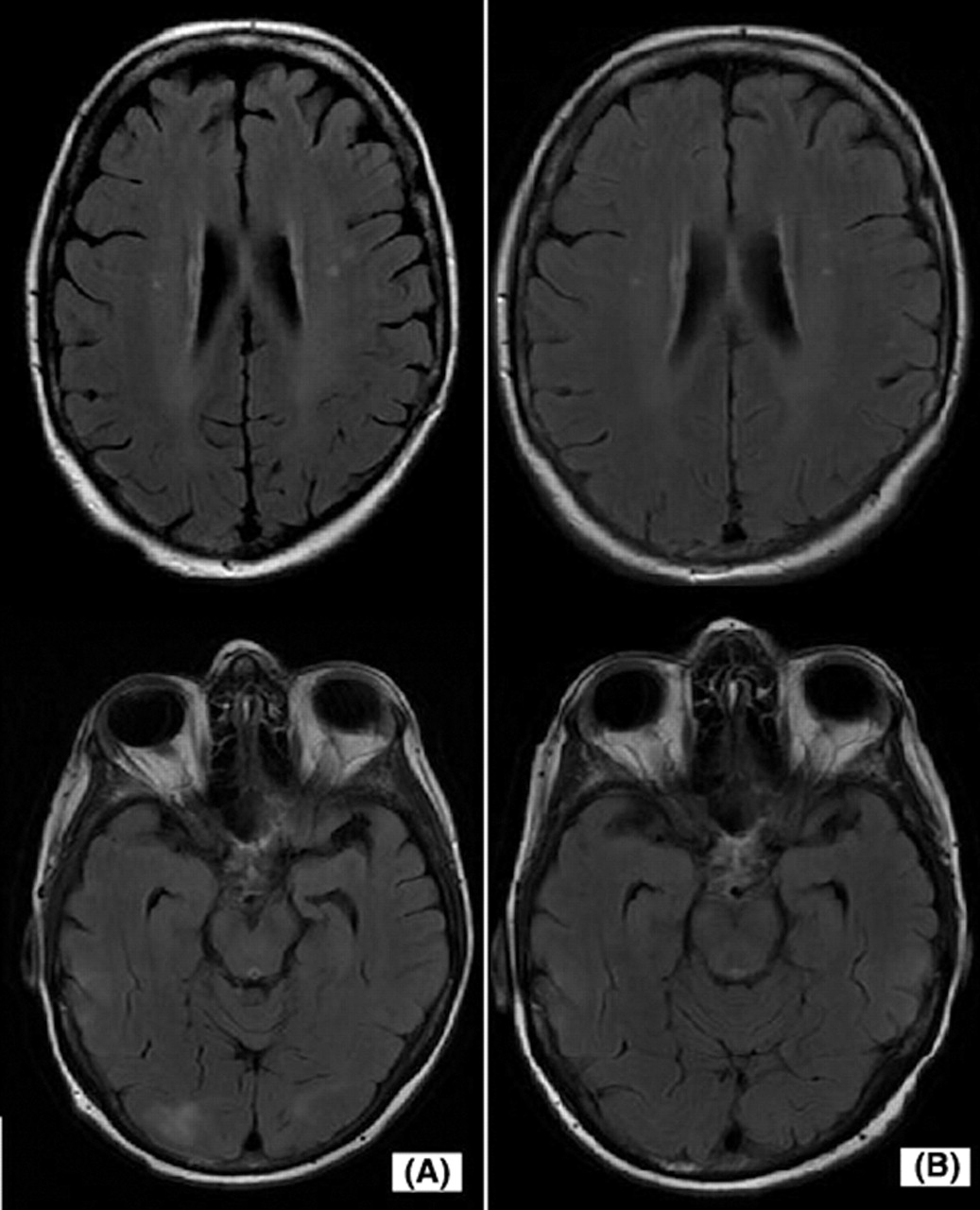
As the name PRES implies, the lesions are predominantly occipital (figure 2). They can be confluent or patchy. Several studies have emphasised the occurrence of atypically located lesions.2 12 13 Indeed, lesions in, for example, the basal ganglia, cerebellum or brainstem can be found in about one-third of cases. But there are only a few case reports with isolated atypically located lesions.12 14 15 Almost all patients (90–98%) have involvement of the parieto-occipital region.8 12 16 The frontal lobe is often affected. A further typical feature is bilateral involvement; in most cases both hemispheres are affected, often asymmetrically. In summary, there is usually a typical PRES pattern of lesions on FLAIR weighted imaging17:
Isolated atypically located lesions are rarely found
As the name implies, the most affected region is the parieto-occipital area
PRES is a leukoencephalopathy but with frequent involvement of the cortex also
Both hemispheres are affected, sometimes asymmetrically.
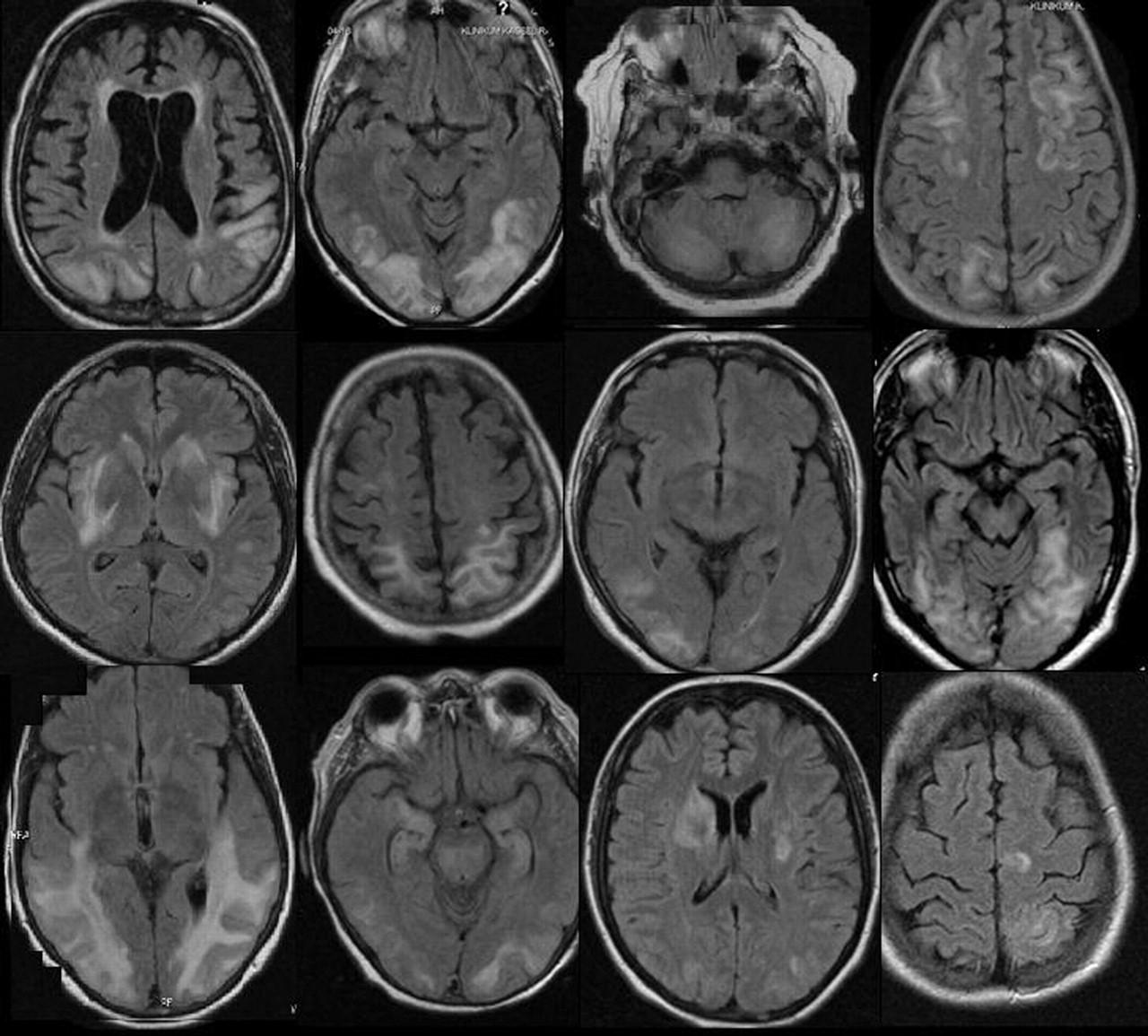
Fluid attenuated inversion recovery weighted MRI of 16 posterior reversible encephalopathy syndrome patients show different lesions. They may be patchy or confluent. Both hemispheres are affected although lesions might be asymmetric.
Intracranial haemorrhage in PRES has recently become better recognised in 15–19% of cases.18 19 Susceptibility weighted MRI (echo planar T2* sequence) is very sensitive in detecting intracerebral haemorrhage and there are three types: parenchymal haematoma, small minute haemorrhages <5 mm, and subarachnoid haemorrhage.18 These mostly occur close to the typical PRES lesions.19 Interestingly, the blood pressure level does not affect haemorrhage frequency which is highest with therapeutic anticoagulation and in patients after allogenic bone marrow transplantation.18 Parenchymal haematoma, in particular, may lead to a permanent deficit and worsen the outcome.8
One theory of the pathophysiology of PRES (see below) is that transient leakage of the blood–brain barrier causes vasogenic oedema but rarely has there been shown to be any leptomeningeal or cortical enhancement on T1 weighted images, and when it has it has been mild.12 20 It is conceivable that this lack of contrast enhancement is due to the timing of the scan, or insensitivity of MRI. Postcontrast FLAIR weighted imaging is not usually performed but it has been suggested to be more sensitive in detecting superficial abnormalities than conventional postcontrast T1 weighted MRI.21 Two recently published case reports have shown enhancement of the subarachnoid space on postcontrast FLAIR imaging, supporting the theory that permeability changes in the blood–brain barrier do occur.21 22
EEG
The EEG is often non-specifically abnormal with diffuse slowing or focal δ waves.23 A study of 28 PRES patients showed EEG slowing in 22 patients and focal sharp waves in three. In another three patients the EEG was normal.3 PRES patients with status epilepticus show rhythmic δ and sharp waves, mostly in parieto-occipital and temporal regions in association with their abnormal imaging findings.9 10 The EEG abnormalities resolve along with clinical improvement.24
Other investigations
Other investigations are not generally helpful except to rule out differential diagnoses (see below).3 Abnormal blood tests may be due to systemic conditions which are associated with PRES—for example, impaired renal function, autoimmune disease or the result of immunosuppressive therapy—but they are not specific for PRES. Laboratory evidence of endothelial injury with thrombocytopenia, red cell fragmentation with schistocyte formation and increased lactate dehydrogenase may be present in PRES patients, especially in pre-eclampsia/eclampsia.25 We did not observe these findings in our own group of PRES patients. Usually all of the blood tests are normal. CSF may be normal or have a slightly raised protein level.
Differential diagnosis
The differential diagnosis of PRES includes severe neurological conditions such as stroke, encephalitis, reversible cerebral vasoconstriction syndrome, intracranial venous thrombosis, intoxication with anticholinergic drugs and primary CNS vasculitis. Although the clinical picture of PRES may not be specific, an early MRI leads to the correct diagnosis in most cases and may, therefore, forestall further investigations.6
Posterior circulation stroke. An important differential diagnosis is the top of the basilar syndrome with infraction in the occipital lobes and brainstem. Like PRES, patients may have visual loss, nausea and other symptoms, but usually no seizures which is a diagnostic clue. Sometimes it can be difficult to decide whether the MR lesions are due to cerebral infarction or PRES. Both infarction and PRES show hyperintensity on FLAIR and T2 weighted imaging. However, thanks to the development of new MRI sequences, especially echo planar DWI and the corresponding apparent diffusion coefficient map (ADC map), it is now possible to differentiate between vasogenic (in PRES) and cytotoxic (in infarction) oedema. Cerebral infarction shows hyperintensity on DWI with low signal on the corresponding ADC map due to the cytotoxic oedema while, in contrast, PRES shows the exact opposite on ADC mapping (figure 3). Some patients may show slightly increased DWI signals without any decrease on the ADC maps, so-called T2 shine through due to increased T2 signal abnormalities, but this does not represent cerebral infarction. In rare cases of PRES, vasogenic oedema may evolve into cytotoxic oedema on follow-up imaging (see below).
Reversible cerebral vasoconstriction syndrome is clinically characterised by thunderclap headache which is not typical for PRES. While PRES quickly progresses over a few hours, complications may occur for several days with the reversible cerebral vasoconstriction syndrome.26 Cerebral angiography may show a ‘string of beads’ but this has also been seen in PRES patients.27 Bilateral parieto-occipital lesions on MRI, typical for PRES, are not characteristic for the reversible cerebral vasoconstriction syndrome. Nevertheless, in about 10% of cases there seems to be overlap between this syndrome and PRES.26
Primary CNS vasculitis. The symptoms usually come on more insidiously and CSF is abnormal, with more than 95% of cases showing an inflammatory reaction. MRI may show multiple infarcts of different ages.
Encephalitis, especially herpes encephalitis, may mimic PRES. The most common symptoms are confusion, seizures and aphasia. Mostly the differentiation is straightforward as in PRES there are no systemic features of inflammation (fever, blood tests, CSF, etc).
Status epilepticus is another cause of reversible MRI lesions. The differentiation between these and those of PRES does not generally cause a problem. Both show hyperintensity on T2 and FLAIR weighted imaging, but in contrast with PRES, in epilepsy the lesions are mainly cortical and only in one hemisphere. Furthermore, DWI shows high signal intensity with slightly low values on ADC mapping. The lesions of course occur in the region of the epileptic focus.28
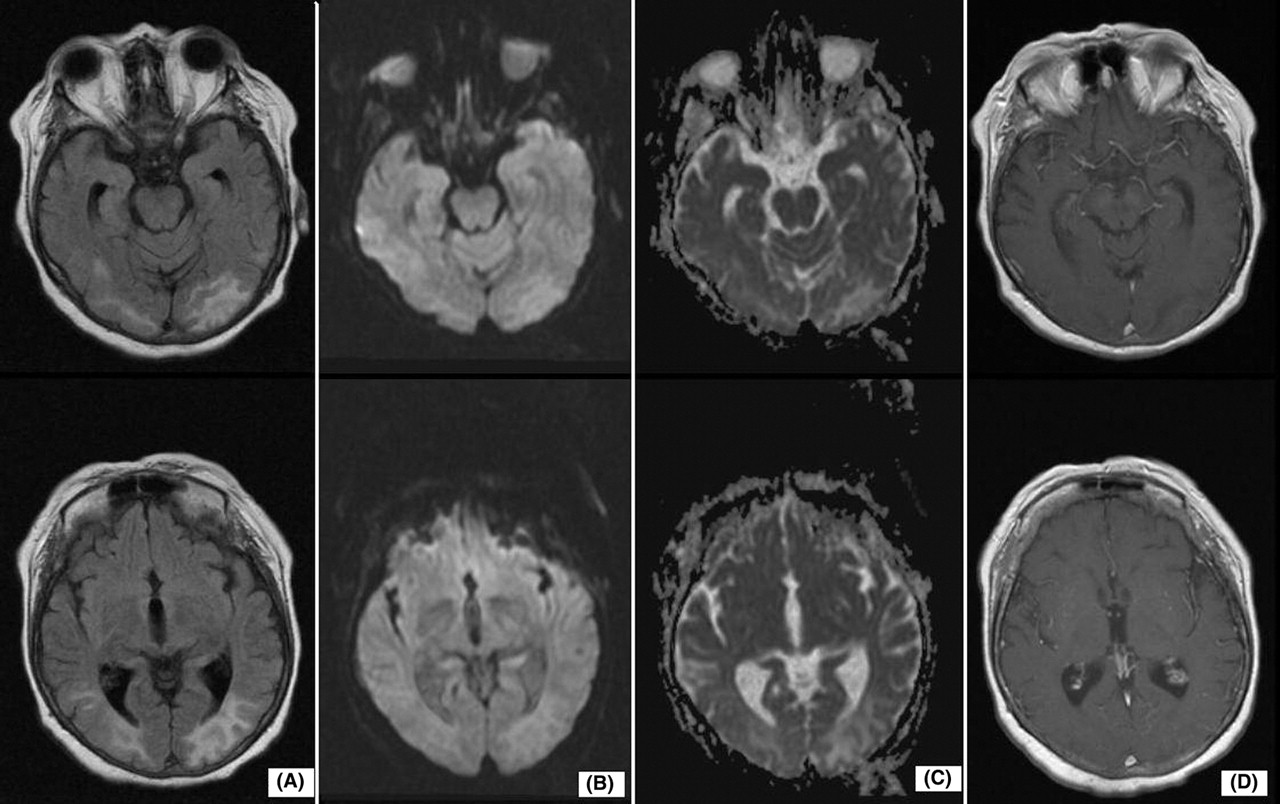
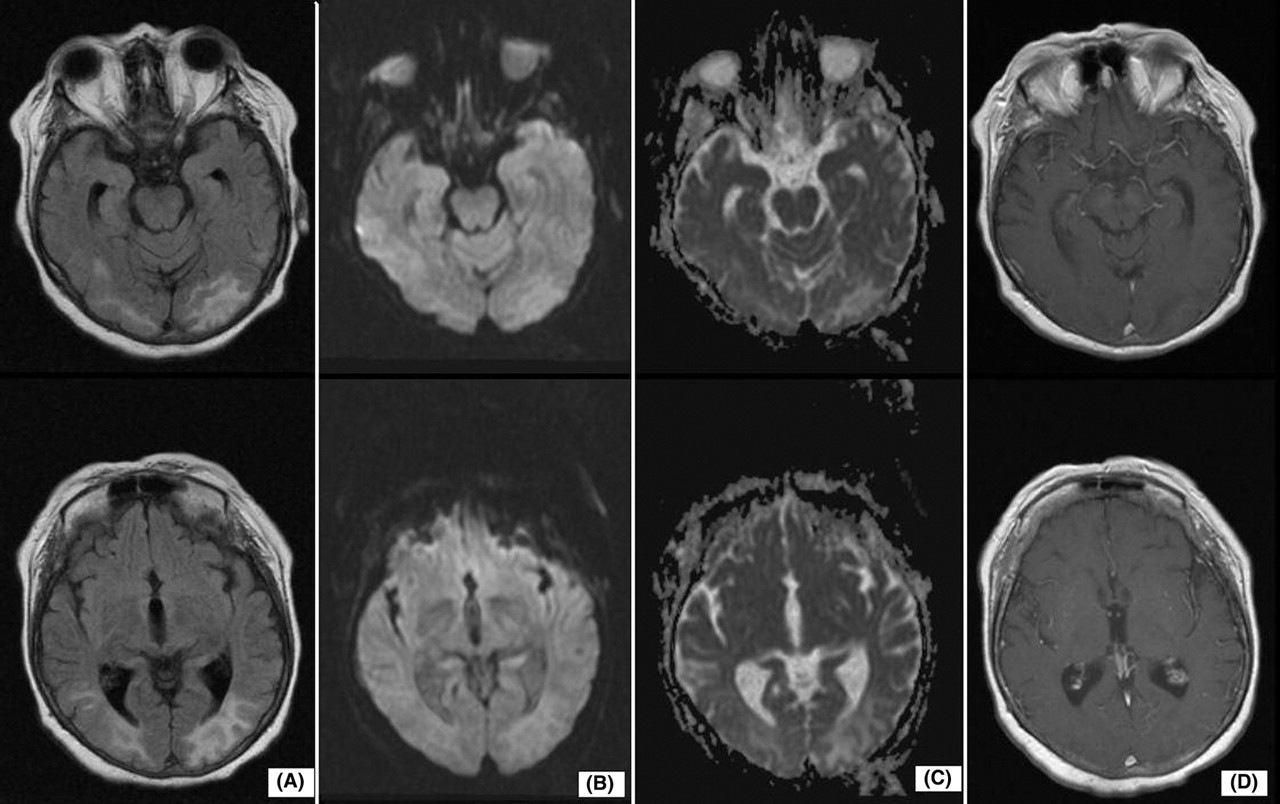
Typical MRI of a posterior reversible encephalopathy shows vasogenic oedema. (A) Fluid attenuated inversion recovery weighted MRI with occipital hyperintensity on both sides. (B) Diffusion weighted imaging is isointense. (C) Apparent diffusion coefficient map shows slightly increased signals occipital. (D) T1 weighted MRI does not show contrast enhancement.
Pathophysiology
There seem also to be many triggers for PRES and there have been various case reports describing different diseases in association with PRES.7 29 The most common triggers seem to be:
Abrupt arterial hypertension
Impaired renal function
Pre-eclampsia/eclampsia; we compared a group of PRES patients who where symptomatic during pregnancy with a group of non-pregnant PRES patients and could not show any difference between the two groups with regard to symptoms, cerebral imaging or outcome. Interestingly, all pregnant women in our study were primigravid4
Immunosuppressive drugs, especially the calcineurin inhibitors such as cyclosporine and tacrolimus. Most PRES episodes due to immunosuppressive therapy occur within 2 weeks of initiation or dose increase; drug serum levels are within the therapeutic range. Nearly 20% of the episodes occur months or years after treatment initiation. PRES should be considered whenever a patient on these medications presents with acute compatible neurological symptoms.30 31 Other cancer chemotherapies have also been described in association with PRES (eg, cytarabine, cisplatin, gemcitabine, bevacizumab)
Transplantation, especially after bone marrow, or stem cell transplantation. This association might be due to the accompanying immunosuppressive therapy. PRES usually occurs within the first month after transplantation
Autoimmune diseases such as systemic lupus erythematosus, Wegener's granulomatosis, systemic sclerosis and polyarteritis nodosa
Infection, particularly with gram positive organisms.
Due to the diverse medical conditions which can lead to PRES, knowledge about this syndrome is important, not only for neurologists but for other physicians too.
The pathophysiology of PRES is poorly understood. There are several theories.
The most popular is that there is breakdown of cerebral autoregulation due to a rapid rise in blood pressure leading to disruption of the blood–brain barrier.1 32 However, blood pressure is normal or mildly elevated in up to 30% of cases and the upper limit of cerebral autoregulation is usually not reached.
A second possibility is endothelial dysfunction due to circulating toxins which is more pertinent for triggers such as immunosuppressive therapy, sepsis, autoimmune disease and pre-eclampsia, which all may affect the blood–brain barrier and lead to subsequent extravasation.29 33 Interestingly, patients on immunosuppressive drugs have lower average blood pressures than other PRES patients.30
The third theory postulates focal vasospasm leading to decreased blood flow and ischaemia with resultant oedema.34
The posterior regions of the brain might be more frequently affected because there is less sympathetic innervation of the blood vessels here compared with the anterior circulation.32
Prognosis
As the name PRES implies, brain lesions are reversible. Nonetheless, occasionally poor neurological outcome has been mentioned again and again as being due to conversion from primary vasogenic into cytotoxic oedema.5 35 36 In our prospective follow-up of 25 PRES patients, poor outcome in three patients was due to multimorbidity (sepsis, dementia) or intracerebral haemorrhage. All other patients had an excellent short term and long term outcome with significant amelioration of their symptoms even while they were still in hospital. We found complete resolution of imaging abnormalities in 72% of cases and all of the others had clear improvement within a mean of 6 weeks of follow-up.8 The symptoms usually seem to resolve in about 3–8 days while recovery of the MRI abnormalities takes longer—several days to weeks8 (figure 4).

A patient in their late 60s who presented with generalised seizures, headache and disturbed vision. The initial blood pressure was 210/130 mm Hg. Clinical symptoms resolved within 2 days. (A) Fluid attenuated inversion recovery weighted MRI on admission shows bilateral hyperintense lesions, parieto-occipital and frontal. (B) On follow-up MRI at day 11, these lesions are still visible. (C) Sixty-seven days after admission the lesions had resolved completely.
Unfortunately, risk factors for irreversible brain damage are unknown but cases with a poor neurological outcome are much less frequent than suggested in the early literature.11
Recovery of the imaging abnormalities confirms the diagnosis and might help differentiate PRES from chronic leukoencephalopathies such as mitochondrial cytopathies, CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy) and metabolic leukoencephalopathies (figure 5). The ideal timing of repeat MRI is about 7–10 days after onset of symptoms when there should usually be clear improvement of the MRI abnormalities.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Fluid attenuated inversion recovery weighted MRI 1 day after admission of a patient with visual disturbance and elevated blood pressure. Changes may be subtle and only reversibility may indicate the nature of the lesion. (B) Follow-up MRI: lesions have resolved thereby allowing distinction between posterior reversible encephalopathy syndrome lesions and other lesions such as subcortical arteriosclerotic encephalopathy or unknown bright objects.
An interesting aspect is the recurrence of PRES. If a particular vulnerability of the brain and certain trigger factors are prerequisites, then one would expect recurring attacks much more frequently than seems to be the case. A retrospective review of PRES cases between 1998 and 2005 suggested recurrent PRES episodes occur in only 4% of cases.37 We have found recurrence in 8% of our 25 patients after complete recovery from their first episode, followed prospectively over a mean follow-up of 4.5 years.8
Management
Management is based on anecdote rather than clinical trials. Most people suggest any trigger factor should be removed—for example, withdrawal of chemotherapy, treating hypertension, caesarean section and intravenous magnesium sulphate for eclampsia, and so on. In our experience, the best management is in an intensive care or intermediate care unit with continuous blood pressure monitoring and intravenous antihypertensive medication. We recommend antihypertensive therapy if systolic blood pressure rises above 160 mm Hg. Aggravation of PRES with nitroglycerin has been described and this drug should, therefore, be avoided.38 Theoretically, corticosteroids should reduce vasogenic oedema but there are no reports of using steroids in the literature. On the other hand, there is a case report of a 4-year-old girl who developed PRES after treatment with steroids for asthmatic attacks.39
PRES is one of the rare diseases that can cause symptomatic epilepsy due to reversible brain lesions. Patients with seizures should be treated with antiepileptic drugs, but for how long is controversial. Although there is a case report of a PRES patient who developed epilepsy despite complete resolution of the MRI lesions,40 seizures do not normally progress to chronic epilepsy.3 8 9 Therefore, we suggest that antiepileptic drugs should not be given for more than 3 months unless there is ongoing epileptic activity on the EEG or recurrent seizures.
Unsolved questions
Although PRES has been known about for more than 15 years, its pathophysiology remains obscure. The prime cause seems to originate in the cerebral vessels. Bartynski and Boardman27 found vascular abnormalities in most of the patients having cerebral angiography with segmental vasoconstrictions, vasodilatations or both, which resolved during follow-up. The increased occurrence of PRES in patients with neuromyelitis optica and positive aquaporine-4 water channel autoantibodies (AQP4) has led to the hypothesis that an alteration in water flux due to AQP4 autoimmunity may predispose to PRES. But a cohort of independently ascertained PRES patients were AQP4 seronegative.41 We suggest that various trigger factors can lead to a pathophysiological process that ends in leakage of the blood–brain barrier, causing vasogenic oedema. We also suggest that the term PRES includes cases of acute hypertensive encephalopathy, a condition which has been recognised for many years.
The role of blood pressure remains unclear. Is raised blood pressure a trigger for PRES or is it only reactive due to the severe neurological condition? Is it true that strict treatment of blood pressure may avoid irreversible lesions due to cytotoxic oedema? Might long term antihypertensive therapy prevent further PRES episodes? Further research, preferably studies with a prospective design, is necessary to solve these questions.
Practice points
PRES is a clinicoradiological syndrome and its symptoms and signs develop over hours—a combination of seizures, disturbed vision, altered mental function and headache.
MRI is the diagnostic gold standard. The predominant affected region is parieto-occipital of both hemispheres. The subcortical white matter is always affected but with frequent involvement of the cortex also. Typical PRES lesions on MRI are thought to represent vasogenic oedema.
Both children and older people can be affected without any gender differences.
There are many different trigger factors, most commonly abrupt hypertension, renal failure, immunosuppressive therapy, eclampsia, autoimmune disease and infections.
The prognosis is good and recurrence rare. Symptoms generally resolve within a week. MRI lesions resolve somewhat more slowly.
Treatment consists of antihypertensive drugs, withdrawal of medication such as chemotherapy, and treatment of any underlying disease.
Acknowledgments
We would like to thank Dr R Siekmann and Dr M Hügens-Penzel, Department of Radiology, for their cooperation. This article was reviewed by Graeme Hankey, Perth, Australia.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.
Other content recommended for you
- Posterior reversible encephalopathy syndrome (PRES): diagnosis and management
- Cerebral-autoregulatory dysfunction syndrome
- Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years?
- Posterior reversible encephalopathy syndrome (PRES): presentation, diagnosis and treatment
- Tumour-like presentation of atypical posterior reversible encephalopathy syndrome with prominent brainstem involvement
- An unusual cause of altered mental status: the importance of monitoring a patient's blood pressure
- Reversible cerebral vasoconstriction syndrome (RCVS) caused by over-the-counter calcium supplement ingestion
- Posterior reversible encephalopathy syndrome associated with the use of chemotherapeutic agents: a rare complication after treatment with vinorelbine
- Posterior reversible encephalopathy syndrome: long-term follow-up
- Posterior reversible encephalopathy syndrome resulting from repeat bortezomib usage