Article Text

Summary
Congenital hernia of the cord, also known as umbilical cord hernia, is an often misdiagnosed and under-reported entity, easily confused with a small omphalocele. It is different from postnatally diagnosed umbilical hernias and is believed to arise from persistent physiological mid-gut herniation. Its incidence is estimated to be 1 in 5000. Unlike an omphalocele, it is considered benign and is not linked with chromosomal anomalies. It has been loosely associated with intestinal anomalies, suggesting the need for a complete fetal anatomical ultrasound evaluation. We present a case of a fetal umbilical cord hernia diagnosed in a 28-year-old woman at 21 weeks gestation. The antenatal and intrapartum courses were uncomplicated. It was misdiagnosed postnatally as a small omphalocele, causing unwarranted anxiety in the parents. Increased awareness and knowledge of such an entity among health professionals is important to prevent unwarranted anxiety from misdiagnosis, and inadvertent bowel injury during cord clamping at delivery.
Statistics from Altmetric.com
Background
Congenital hernia of the cord, also known as an umbilical cord hernia, is often mistaken for an ‘omphalocele minor’.1 It is thought to arise from persistence of physiological herniation of the mid-gut beyond 10–12 weeks gestation.2 Umbilical cord hernia is different from postnatally diagnosed umbilical hernia, in that the contents of the sac never returned inside the abdominal cavity.3 Its incidence is estimated to be about 1 in 5000.4 Owing to the lack of awareness of this entity, it is often misdiagnosed and under-reported, with limited data in the literature.
Umbilical cord hernias are thought to be benign with favourable outcomes, and an isolated presentation of an umbilical cord hernia has not been associated with other chromosomal anomalies.5 An omphalocele, on the other hand, is a more concerning prenatal ultrasound finding. Omphaloceles are usually characterised by a large umbilical defect resulting from a failure of closure of the ventral abdominal wall and is associated with other chromosomal anomalies, in turn having poorer prognosis.5 About 30–40% of fetuses with omphalocele have an abnormal karyotype, and 50–70% of them have other major anomalies such as pentalogy of Cantrell, amniotic band syndrome, schisis association, OEIS syndrome (omphalocele, exstrophy of the bladder, imperforate anus, spinal defects), Shprintzen syndrome, Carpenter syndrome, Goltz syndrome, Marshall-Smith syndrome, Meckel-Gruber syndrome, otopalatodigital type II syndrome, CHARGE syndrome and Beckwith-Wiedemann syndrome.6–8
Increased awareness and knowledge of umbilical cord hernia is important to prevent unwarranted parental anxiety from misdiagnosis and inadvertent bowel injury during cord clamping at delivery.
Case presentation
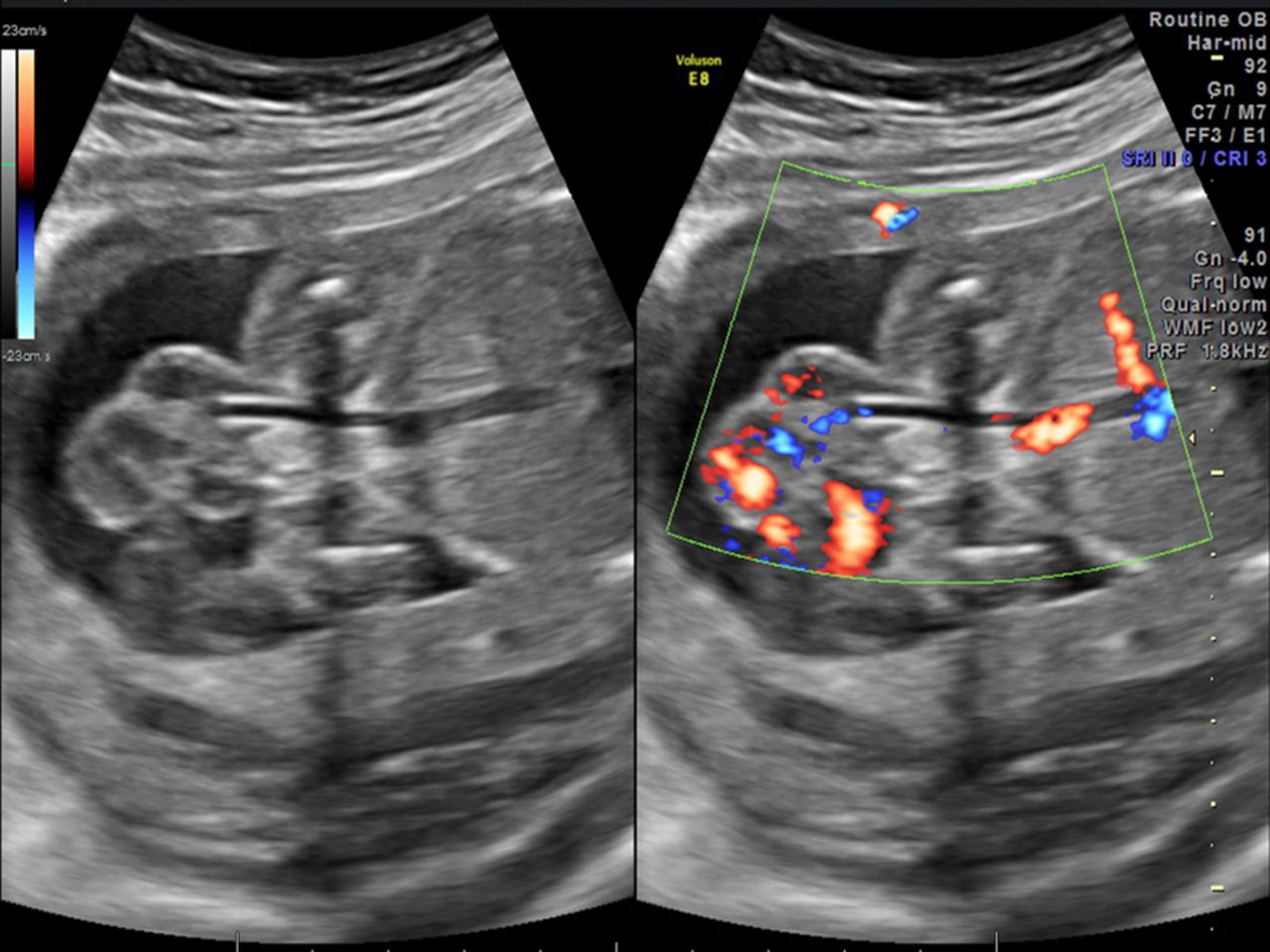
A 28-year-old woman, gravida 2, para 0, presented to our clinic at 21 weeks gestation for routine prenatal care. Her initial obstetrical ultrasound showed findings consistent with a fetal umbilical cord hernia. A loop of small bowel was noted to be extending into the base of the umbilical cord, measuring 4.48 cm×2.71 cm (figures 1⇓⇓–4). The placenta was noted to be low lying, about 1.7 cm from the internal cervical os. The patient was counselled about the benign nature of the findings and the importance of follow-up ultrasound examinations.

Sagittal section of the umbilical cord at its abdominal wall insertion site.

Sagittal section of the umbilical cord at its abdominal wall insertion site with colour Doppler.

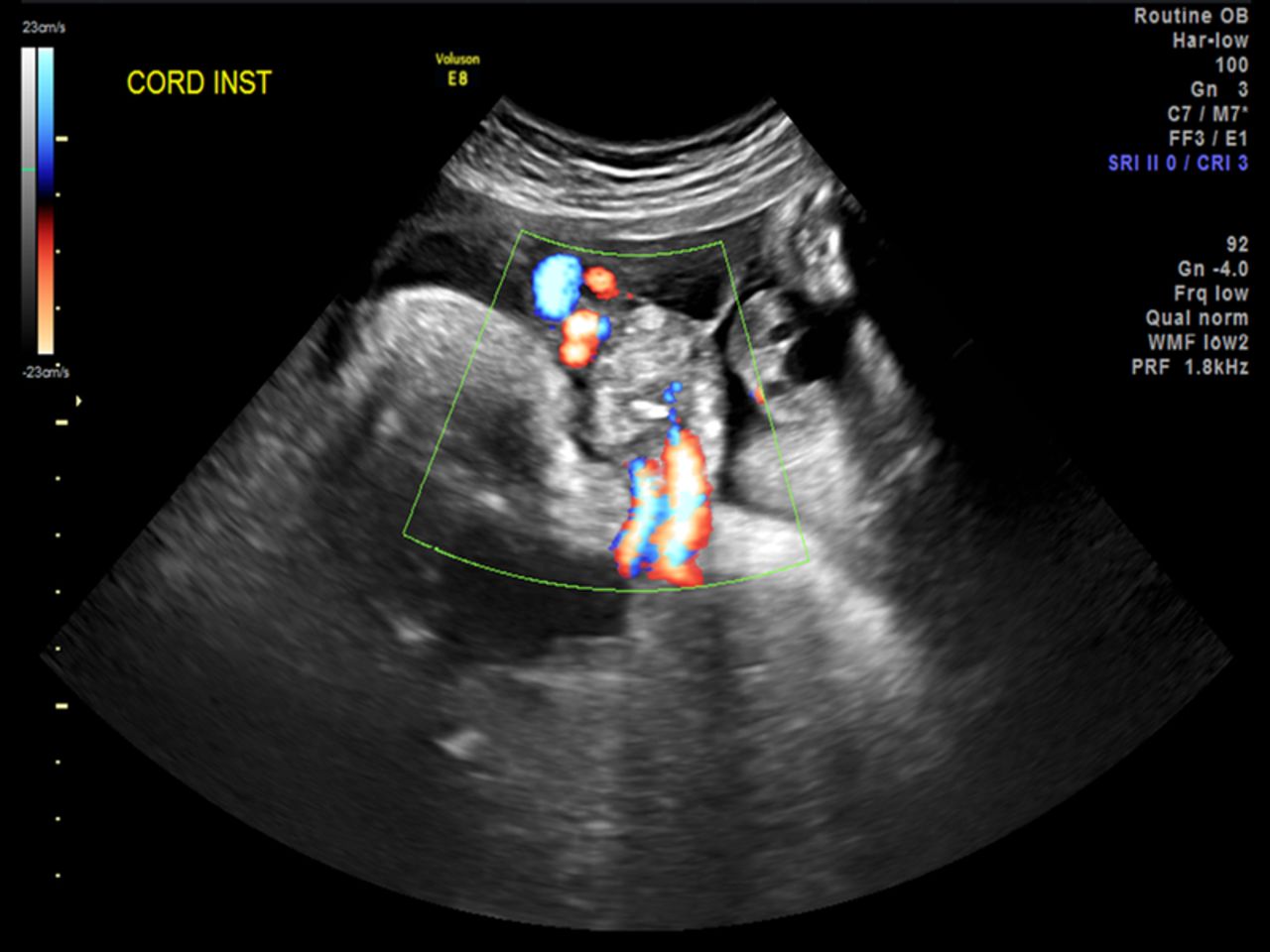
Cross-section of the umbilical cord showing the umbilical cord cyst.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cross-section of the umbilical cord at its abdominal wall insertion site with colour Doppler.
Her obstetrical history was complicated with late prenatal care. Her medical and surgical histories were unremarkable. She quit smoking 2 years earlier but used to smoke 2 packs per week for about 5 years (1.5 pack years). She was a social drinker and denied any history of illicit drug abuse.
Investigations
A subsequent obstetrical ultrasound 4 weeks later noted the persistence of the fetal umbilical hernia with a new finding of a simple appearing cord cyst measuring 2×2 cm directly adjacent and distal to the umbilical hernia (figure 3). A fetal echocardiogram was performed to complete the fetal anatomical evaluation, which was also unremarkable. Follow-up obstetrical ultrasounds every 4 weeks showed normal fetal growth and amniotic fluid volume, with persistence of the umbilical cord hernia and cyst. We counselled the patient about the benign nature of the condition, especially in the absence of any other fetal anomalies. Diagnostic amniocentesis was not performed as the ultrasound findings were highly suggestive of an umbilical cord hernia. Antepartum fetal surveillance was started at 36 weeks’ gestation with weekly non-stress testing and amniotic fluid index measurements in view of late prenatal care. Fetal well-being remained reassuring.
Differential diagnosis
The differential diagnosis for the obstetrical ultrasound findings include other ventral wall defects such as omphalocele and gastroschisis (table 1). In our case, the ultrasound findings of the small bowel extending into the base of the normally inserted umbilical cord were highly suggestive of an umbilical cord hernia. On ultrasound, an omphalocele usually presents as a fetal midline abdominal mass with the umbilical cord attaching at the apex of the mass.8 Gastroschisis usually presents with ultrasound findings of exteriorised bowel, in relation to the anterior abdominal wall, floating freely in the amniotic cavity adjacent to a normally inserted umbilical cord.9
Differential diagnosis of ventral wall defects
Treatment
Pregnancy was largely uncomplicated, except for a mild episode of shortness of breath, which was consistent with symptoms of allergic rhinitis. At 41 weeks 1 day, the patient went into active labour and delivered a 7 lb 8 oz (3550 g) female baby. During the delivery, the umbilical cord was cut long in order to prevent injury to the bowel. Neonatology was present for the delivery and the baby was taken to the neonatal intensive care unit in preparation for operative repair of the defect. Paediatric surgery was consulted on the day of delivery and they diagnosed the baby with a ‘small omphalocele’. Chromosome analysis, echocardiogram and cranial ultrasound were ordered, and all returned unremarkable. The baby was placed on total parenteral nutrition and underwent primary fascial closure with umbilicoplasty on day 1 of life.
Outcome and follow-up
The postpartum course for the mother was uncomplicated. The baby had an uncomplicated postoperative course and was subsequently discharged home on day 6 of life. The mother presented to us at her 6-week postpartum visit with her baby. Her baby was noted to be doing well.
Discussion
Umbilical cord hernia was first described in the literature by Hempel-Jorgensen15 in 1929. It is thought to be under-reported and often misdiagnosed as an ‘omphalocele minor’ due to similarities in appearance.1 Clinically, it can be distinguished from an omphalocele by the umbilical cord insertion site.2 ,6 In an umbilical cord hernia, there is a normal cord insertion with intact skin covering the umbilical ring. An omphalocele, on the other hand, is characterised by a large defect in the umbilical ring involving the skin and muscle, often covered by amniotic membrane that may contain bowel and other viscera such as the liver, with an umbilical cord insertion on top of the herniated sac.2
Klein et al5 described umbilical cord hernias as being associated with intestinal malrotation. Pal et al1 described them as being associated with persistent vitello-intestinal duct, cloacal anomalies and intestinal atresia. Haas et al described them as being associated with umbilical cord cysts, intestinal dilation and ascites, and hyperechoic short bowel. They also report one case of intrauterine fetal death a few weeks following identification of bowel dilation and ascites.6 Owing to the limited number of studies, these associations have not yet been proven. Larger studies are needed to validate these associations. We still feel it is important to do a complete fetal anatomical ultrasound evaluation when presented with an umbilical hernia. Haas et al,6 in their case series of eight patients with umbilical cord hernia, the largest study to date, recommended that umbilical cord hernia associated with bowel complications undergo close monitoring and early induction of labour between 34 and 36 weeks’ gestation. Postnatally, umbilical cord hernias are usually managed with primary surgical closure.2 ,5 Overall, the prognosis of an isolated finding of umbilical cord hernia is better than for an omphalocele.5 ,6
Prenatal diagnosis is important to prevent inadvertent injury to the bowel during cord clamping at the time of delivery.6 We had a similar case of an umbilical cord hernia at our institution in the past, but undiagnosed, which resulted in an enterotomy during cord clamping. It is important to cut the umbilical cord distant from the abdominal site of insertion. A safe distance to clamp can be determined from evaluation of prenatal ultrasounds and palpation of the cord during the time of delivery.
Increased awareness and knowledge of umbilical cord hernias among health professionals is important to prevent unwarranted anxiety from misdiagnosis and inadvertent bowel injury during cord clamping at delivery.
Learning points
-
Congenital hernia of the cord, also known as an umbilical cord hernia, is an often misdiagnosed and under-reported entity easily confused with a small omphalocele.
-
Unlike omphaloceles, umbilical cord hernias are benign entities not associated with any chromosomal anomalies, thus having a better prognosis.
-
Prenatal diagnosis of an umbilical cord hernia and knowledge of it is important to prevent unwarranted parental anxiety.
-
The umbilical cord should be clamped distal to the abdominal site of insertion to prevent inadvertent bowel injury at the time of delivery. A safe distance to clamp can be determined from evaluation of prenatal ultrasounds and palpation of the cord.
Acknowledgments
The authors acknowledge Doug Pike for helping with the image formatting.
Footnotes
-
Contributors QL and MS were involved in writing the article. IV is the mentor and guided throughout the writing process, and in proof reading and reviewing the article.
-
Competing interests None declared.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.