Article Text

Abstract
Objective To determine the relationship of disease activity to infections in patients with rheumatoid arthritis (RA).
Methods From the CORRONA database, the incidence of physician-reported infections in RA patients on stable disease-modifying antirheumatic drug, biological, and corticosteroid therapy for at least 6 months was ascertained. Two composite measures of disease activity were defined: clinical disease activity index (CDAI) and disease activity score 28 (DAS28). Incident rate ratios (IRR) were calculated using generalised estimating equation Poisson regression models adjusted for demographics, medications and clinical factors.
Results Of 1 6242 RA patients, 6242 were on stable therapy for at least 6 months and were eligible for analysis. 2282 infections were reported in the cohort, followed over 7290 patient-years. After controlling for possible confounders, disease activity was associated with an increased rate of infections. Each 0.6 unit increase in DAS28 score corresponded to a 4% increased rate of outpatient infections (IRR 1.04, p=0.01) and a 25% increased rate of infections requiring hospitalisation (IRR 1.25, p=0.03). There was a dichotomy in the relationship between infections and CDAI scores. For CDAI <10 (mild disease activity) patients had a 12% increased rate of outpatient infections with each 5 unit increase in CDAI score (IRR 1.12, p=0.003). At CDAI scores ≥10, there was no further increase in the rate of outpatient infections associated with higher disease activity. The relationship of CDAI to hospitalised infections showed similar trends to outpatient data but did not reach statistical significance after multivariate analysis (CDAI <10: IRR 1.56, p=0.08).
Conclusions In this large cohort of RA patients, higher disease activity was associated with a higher probability of developing infections.
Statistics from Altmetric.com
Infections are a frequent complication in patients with rheumatoid arthritis (RA) and contribute to increased morbidity and mortality. Numerous studies have illustrated the increased risk of infections in RA patients,1 2 and patients with RA seem particularly vulnerable to pulmonary infections.3 RA patients are at a twofold increased risk of developing infections and are also at higher risk of serious infections requiring hospitalisation.2 The continued increased mortality observed in RA patients compared with the general population4 can be explained partly by a higher susceptibility to infections.5,–,12
Infectious adverse events are frequent in both clinical trials and in practice, and that frequency may vary due to specific RA therapies, disease activity, or other factors. The independent contribution of RA disease activity and associated systemic inflammation is unclear. We therefore sought to determine if there was an association between disease activity and the rate of outpatient and hospitalised infections among RA patients, after accounting for other confounding factors.
Patients and methods
Data were prospectively collected between March 2002 and December 2007 from patients enrolled in the Consortium of Rheumatology Researchers of North America (CORRONA) registry. The CORRONA registry is a multicentre longitudinal study of rheumatology patients that includes patients with RA, psoriatic arthritis and osteoarthritis. The CORRONA registry includes both academic and private practices and data are contributed by more than 80 sites across the USA as of November 2008.13
All CORRONA registry patients enrolled between March 2002 and December 2007 with a rheumatologist-reported clinical diagnosis of RA were included. Patients with overlapping psoriatic arthritis and RA were excluded. To minimise confounding related to recent changes in disease-modifying medications on the rate of infections we limited the study to RA patients on stable therapy. Stable therapy was defined as no change in the dose of methotrexate, tumour necrosis factor (TNF) inhibitor, corticosteroid therapy, or any other disease-modifying antirheumatic drug (DMARD) (excluding methotrexate, TNF inhibitor, or prednisone) during three consecutive visits. Patient and physician questionnaires were completed approximately every 4 months. Data collected include demographic information, disability status (as determined by the treating physician), medical history, medications, tender joint count, swollen joint count, patient global assessment, physician global assessment, laboratory data (including erythrocyte sedimentation rate (ESR)), modified patient health assessment questionnaire disability index (mHAQ), patient visual analogue scale (VAS) for pain, hospitalisations, infections and medical insurance. Medical insurance for patients in the CORRONA database was provided by Medicaid (government-run insurance for low-income patients), Medicare (government-run insurance for patients >65 years old or with disability), or private insurance.
Disease activity measurements
Two composite measures of disease activity were examined: the clinical disease activity index (CDAI, range 0–76) and the disease activity score 28 (DAS28). CDAI sums swollen 28 joint counts, tender 28 joint counts, patient global assessment (range 0–10), and physician global assessment (range 0–10).14 The CDAI score can be divided into low (CDAI <10), moderate (CDAI 10–22), and high (CDAI >22) disease activity.15 DAS28 is a computation of disease activity that includes weighted measures of swollen 28 joint counts, tender 28 joint counts, ESR and the patient global assessment.16 DAS28 values were limited to patients who had valid ESR values within 2 weeks of the patient visit analysed. Disease activity by DAS28 is divided into low (<3.2), moderate (3.2–5.1) and high (>5.1) disease activity. The minimal clinically important difference for detecting a change in disease activity was determined as a change in the CDAI of 5 units and a change in the DAS28 of 0.6 units.17
Infection definitions
The occurrence of outpatient and hospitalised infections was identified by the treating rheumatologist in case report forms at each visit. Given that there are no well agreed-upon case definitions for outpatient infections in the medical literature, infections were identified based upon the physician's report according to standard of care. CORRONA does provide a means to categorise infection, which included infection sites (joint, sinusitis, etc) and pathogens, when known, (eg, Herpes zoster, listeria, tuberculosis, etc). For hospitalised infections, the patients' charts and hospital records were examined (medical records available 64% of the time) to confirm the validity of the infection.18
Statistical analysis
The relationship of predictor variables to the incidence of infectious adverse events was analysed using incidence rates (per 100 person-years) and estimated using incidence rate ratios (IRR). Generalised estimating equation Poisson regression models were used to estimate unadjusted and adjusted IRR with 95% CI. This modelling framework provided appropriate estimates and CI accounting for correlations due to multiple time intervals per patient and the time-varying nature of disease activity. The regression model also allowed adjustment for possible confounders including: demographics (gender, age, body mass index (BMI), education, race (white vs others), insurance, marital status, and smoking hx), co-existing cardiovascular disease (CVD), mHAQ, VAS, duration of RA, severity of RA (designated by the physician on a 1–5 scale at time of enrollment), history of infections and current stable therapy (methotrexate, TNF inhibitors, prednisone, and/or other DMARD (other than methotrexate, TNF inhibitors and prednisone)). Variables significant in univariate analysis (p≤0.05) were included in the multivariate regression models with the exception of pain (patient VAS). Patient VAS for pain was excluded from the multivariable models because it was highly correlated with the CDAI and DAS28.
‘Baseline’ was defined at the third consecutive CORRONA visit with stable RA medications, and any infections and hospitalisations noted at and following the third CORRONA visit were included in the study. Observation time to identify infections therefore began after the second CORRONA visit. The time-varying covariates of interest (DAS28, CDAI, mHAQ, VAS) were updated at each subsequent CORRONA visit. We censored patients at the time they experienced an outpatient or inpatient infection or if they changed RA medications. We also censored patients if they experienced a hospitalisation for reasons other than an infection, as medications often change due to the hospitalisation. For the outpatient infection outcomes we also excluded visits immediately following any hospitalised infections. Patients could contribute more than one episode of observation to the study if they met the three visit stable RA medications criterion after having previously been censored.
The linear association of the outcome and covariates was examined using lowess curves.19 A lowess curve is a locally weighted scatterplot smoothing curve that fits a regression model at each point and results in a non-parametric smoothing curve to fit the data. A non-linear association of infections and CDAI was observed visually and a linear spline model with a knot at CDAI 10 was estimated. This allows a different estimate of IRR above and below 10. A similar spline model was examined for DAS with a knot at DAS 3.2. We also examined a knot at 20 for CDAI and 5.1 for DAS. To test whether a spline relation provided a better fit compared with a simple linear relation, we compared models with knots at the join points described above with those without knots and compared changes in a generalised estimating equation version of Akaike's information criterion, the quasi-likelihood information criterion.20 Statistical analyses were done using Stata version 10.1.
Results
A total of 16 242 RA patients with 80 691 visits was identified. Of these, 6246 patients with a total of 19 790 visits on stable therapy were included in the study. The average follow-up time per patient was 1.2 (± 0.9) years, the average time between visits was 4.4 (±2.3) months. A total of 6020 patients had CDAI scores while 3666 patients had DAS28 scores calculated. The number of patients who had DAS28 scores was lower because of the unavailability of ESR data (within 2 weeks of the visit) for many of the patients. A total of 2354 patients only had CDAI available for this study. The baseline characteristics of the patients are shown in table 1. The mean age of the patients was 60.2 years (±13.1) and 74.5% were women.
Baseline† characteristics of rheumatoid arthritis patients on stable therapy (n=6246)
A total of 2282 infections was reported in this cohort of RA patients. The overwhelming majority of infections was outpatient infections; there were 2223 outpatient infections that occurred during 7115 person-years of stable therapy. A total of 1382 patients had an outpatient infection and 50 patients had hospitalised infections in this cohort. The event rate for outpatient infections was 31.2 events per 100 person-years (table 2). In cases in which a site of infection was identified, the most common outpatient infections reported were upper respiratory infections/pneumonias, followed by sinusitis and urinary tract infections (UTI). The total number of infections per disease activity category is shown in table 3.
Number of infectious adverse events and incidence rates (per 100 person-years) for patients on stable therapy
Incidence of infections within disease activity categories
Relationship of disease activity to infection rate
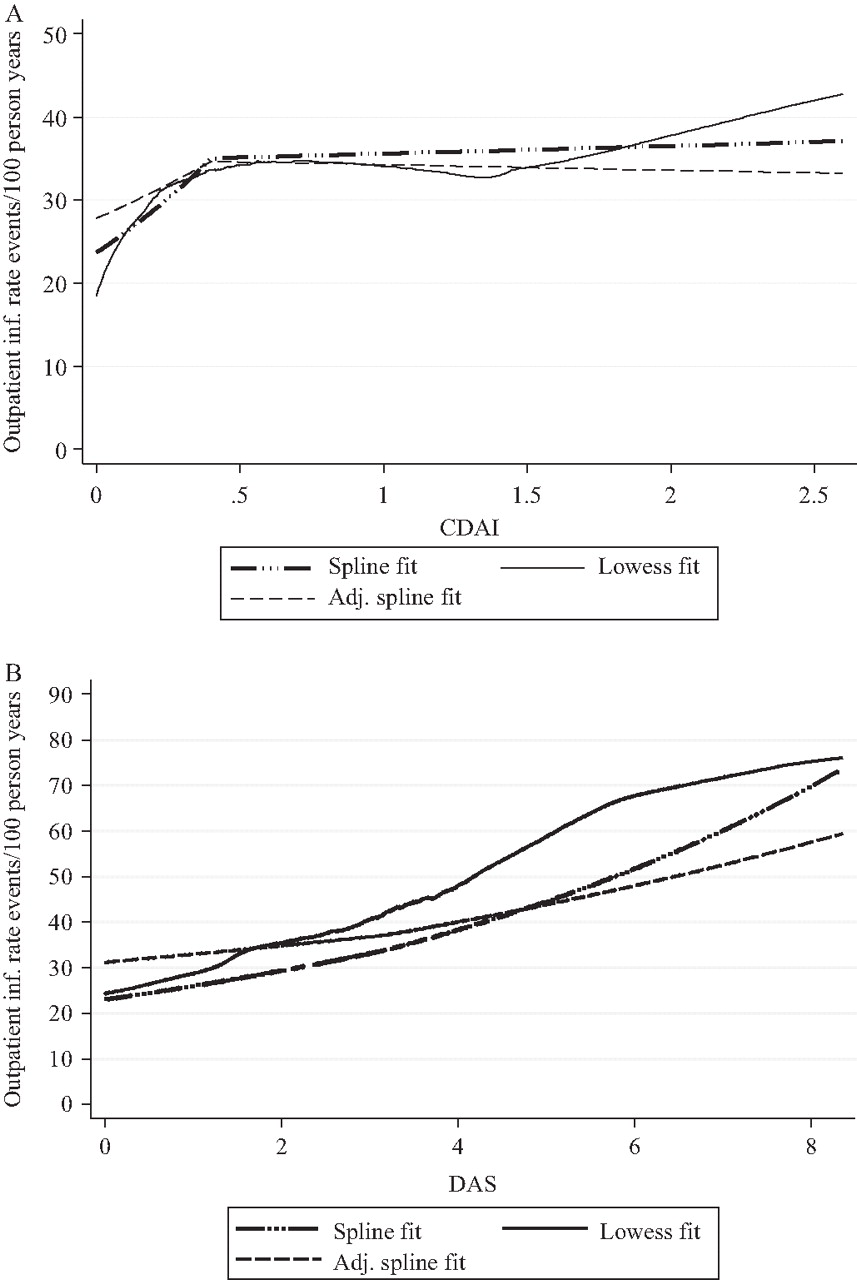
In this population of RA patients receiving stable therapy, we found that the relationship of CDAI to infection rate was non-linear (figure 1A). A spline model with a knot at CDAI 10 provided a better fit of the data than a model without the knot, indicating the IRR differed across the range of disease activity when CDAI was in the mild range (<10) versus the moderate–severe range (≥10). We also examined a spline model with a knot at CDAI 20, but the IRR for the infection rate was not significantly different between a CDAI less than 20 and CDAI of 20 or greater. Unlike CDAI, the association of DAS28 with outpatient infection appeared to be linear (figure 1B).
{kind=link}
(A) Spline and lowess fit models for clinical disease activity index (CDAI) and rates of outpatient infections. (B) Spline and lowess fit models for disease activity score 28 (DAS28) and rates of outpatient infections.
Univariate analyses for outpatient and hospitalisation-requiring infections
Univariate analyses for outpatient infections and hospitalised infections are shown on table 4. Disease activity, as measured by the CDAI and DAS28, was significantly associated with an increased rate of outpatient infections and infections requiring hospitalisation in univariate analyses.
Unadjusted generalised estimating equation Poisson analysis for infections
Adjusted analysis outpatient infections
Adjusted CDAI and DAS28 models for outpatient infections are shown in table 5.
Adjusted generalised estimating equation Poisson analysis for outpatient infections
In mild disease activity CDAI range, each 5-unit increase in CDAI correlated to a 14% increase in outpatient infections after adjusting for all significant covariates (IRR 1.14, p=0.003). No further increase in outpatient infections was noted with CDAI scores above 10 (IRR 1.00, p=0.99). There was a 4% increase in outpatient infections for each 0.6-unit increase in DAS28 (IRR 1.04, p=0.03). When we repeated our CDAI analysis, restricted to only the patients and observation periods that corresponded to the data used for the DAS28 analysis, we found similar results in the relationship of CDAI and infections. In the subgroup of CDAI patients with DAS28 scores available, the adjusted IRR for outpatient infections was 1.15 (95% CI 1.03 to 1.29) for CDAI less than 10, and no further increase in outpatient infections was noted at CDAI scores of 10 or greater (IRR 1.00, 95% CI 0.95 to 1.06). These estimates are similar to those for the entire CDAI cohort (table 5). We performed a sensitivity analysis by examining the relationship of CDAI with outpatient infections when broken down into categories of low disease activity (CDAI <10), moderate disease activity (CDAI 10–22) and high disease activity (CDAI >22). Patients with moderate and high CDAI disease activity had increased infections when compared with patients with low disease activity, but only moderate disease activity was statistically significant (IRR for outpatient infections: CDAI <10, IRR 1; CDAI 10–22, IRR 1.19 (95% CI 1.06 to 1.34); CDAI >22, IRR 1.07 (0.90 to 1.27)).
A history of infections increased the likelihood of having an outpatient infection (IRR 2.84–3.15, p<0.001). Other factors associated with outpatient infections included methotrexate use, TNF inhibitor use and poorer functional class.
Adjusted analysis for infections requiring hospitalisation
Adjusted CDAI and DAS28 models were estimated for hospitalised infections and are reported in table 6. Given the small number of hospitalised infections, we limited our adjusted analysis to covariates that were statistrically significant in the full model. Disease activity, as measured by the DAS28, was associated with a rate of infections requiring hospitalisation after adjusted analysis. Each 0.6 increase in the DAS28 was associated with a 25% increased rate of infections requiring hospitalisation. The association of CDAI with hospitalised infections did not reach statistical significance. However, the IRR for CDAI in the under 10 unit range was numerically greater than for the outpatient infection analysis. Prednisone use of 7.5 mg daily or greater was associated with increased infections requiring hospitalisation. Increased hospitalised infections were also associated with a history of any infection and a history of hospitalised infection in the CDAI model.
Adjusted generalised estimating equation Poisson analysis for infections requiring hospitalisation
Discussion
Previous reports show that there is an increased incidence of infections in RA patients compared with non-RA patients1,–,4 21 22 but the relationship of infection risk and RA disease activity has been largely unexplored. We found in this large US cohort of RA patients receiving stable DMARD, biological and/or corticosteroid therapy, that increasing disease activity is associated with a higher probability of developing infections, although other factors such as medications may affect the incidence of such infections. After multivariate analysis, higher disease activity, as measured by the CDAI or DAS28, was associated with an increased rate of outpatient infections. The DAS28 was also associated with increased hospitalised infections. Patients with mild disease activity (CDAI <10) had a 14% increase in outpatient infections per 5-unit increase in CDAI score. Higher disease activity, as measured per 0.6 units in the DAS28 score, corresponded to a 4% increase in outpatient infections and a 25% increase in hospitalised infections. Disease activity as measured by the CDAI was significantly associated with increased hospitalised infections in bivariate analysis but not in multivariate analysis. This may have been due to insufficient power as the number of hospitalised infections was relatively small (59 out of a total of 2282 infections). One other study found no association between disease activity (DAS28) and infection rate,23 but did note an association with HAQ scores (IRR 1.75). We found that the mHAQ scores correlated with the infection rate in univariate analysis, but did not remain significant in the multivariate analyses.
The relationship of the CDAI with the infection rate was non-linear (figure 1A), and spline analysis was performed to allow a different estimate of IRR above and below a CDAI of 10. We noted a difference in the association of rising disease activity scores to infection rate in patients with mild disease activity compared with moderate/severe disease activity. In patients with mild disease activity, increasing CDAI correlated with an increased rate of outpatient infections. The association between the CDAI and outpatient infections appeared to plateau (figure 1A) once patients have moderate or severe disease activity. In contrast, the relationship of the DAS28 with the infection rate appeared to be linear (figure 1B). More patients were included in the CDAI model than the DAS28 model due to the lack of timely ESR values for all patients.
To evaluate whether the difference in the CDAI and DAS28 models were due to a selection bias, we reanalysed the CDAI models using only the subgroup that also had a DAS28 score available. Similar results were obtained in this subgroup analysis. The individual components of the CDAI and DAS28 were examined to determine why the two indices of disease activity correlated differently to infection rates. We discovered that the relationship of tender 28 joint counts to infection was very similar to CDAI, in that tender 28 joint counts increased with the infection rate at low scores but plateau with higher counts. Baseline differences between patients who had DAS28 scores and patients with CDAI scores but no DAS28 may explain the different relationships of CDAI and DAS28 to infections (table 1). Patients with DAS28 scores were less disabled, had lower CRP and HAQ scores, used more methotrexate and TNF therapies, and had lower prednisone and other DMARD use. The inclusion of ESR in the DAS28 calculation may also have contributed to the differences noted between the CDAI, DAS28, and their effects on the infection rate in RA. Alternatively, as there were fewer patients with DAS28 than CDAI scores, there may not have been sufficient power to detect a difference in infections between low and higher disease activity in our DAS28 model.
The rate of outpatient infections observed in this cohort (31.2 per 100 person-years) is comparable to that observed in the retrospective longitudinal study by Doran et al.1 Our rate of infections requiring hospitalisation is lower than that observed in other studies in RA. We observed a rate of 0.8 infections requiring hospitalisation per 100 person-years. Dixon et al23 found infections requiring hospitalisation rates of 4.1–5.3 per 100 patient-years while Smitten et al2 found rates of 3.8 per 100 patient-years. The rates of infections that required hospitalisation may have been lower in our study because we restricted our analysis to patients who were on stable therapy. The methodology of the studies may have also contributed to the difference in hospitalised infection rates. Dixon et al23 used patient diaries with confirmation by the rheumatologists while Smitten et al2 used a claims database. Our hospitalised infections were documented by record review and thus some non-infectious hospitalisations or non-proved infections were excluded and decreased the apparent rate of hospitalised infections.
We observed that different classes of medications were associated with different types of infections. Patients on 7.5 mg or more of daily prednisone had greater than six times the rate of infections requiring hospitalisation after controlling for multiple confounders including disease activity. Our findings are consistent with many other studies, which showed that corticosteroids increase the rate of serious infections in RA patients.2 24,–,28 We found an increased rate of outpatient infections with stable TNF inhibitors. TNF inhibitors have been associated with an increased risk of infections,29 30 particularly respiratory tract infections.31 32 Patients on low-dose methotrexate had more outpatient infections, and other studies have found an increased risk of infections with methotrexate use.24 29
A previous history of infection was significantly associated with an increased rate for both outpatient and hospitalised infections in this study. This is consistent with other studies, which found an increased infection rate in patients with a previous history of infections.25 27 Poor functional class also contributed to increased outpatient infections in this cohort. Other risk factors for increased outpatient infections in this cohort included female gender, younger patients and those with history of CVD.
The strengths of this study are attributable to the size and quality of the clinical data. The CORRONA database represented a large and diverse sample of clinical patients from 80 sites across the USA. In this registry, all data were prospectively collected, with infection and medication data recorded by the treating rheumatologist at the time of the visit. Furthermore, we reviewed the patients' hospital records to confirm the status of infections requiring hospitalisation.
This study has several potential limitations. All data from the CORRONA database were obtained by questionnaires completed at the time of a clinical encounter, and there is the potential for an underascertainment of infectious events. There is also the possibility that residual confounding factors persisted despite our adjustment for multiple covariates.
In conclusion, we report that higher disease activity as measured by the DAS28 and CDAI was associated with an increased rate of infections in RA patients on stable therapy. Higher disease activity was associated with an increase in the rate of outpatient and hospitalised infections. A previous history of infection was an independent risk factor for both outpatient and hospitalised infections in this cohort. Medications may also confer risks. We observed higher rates for hospitalised infections with patients on corticosteroids and higher rates of outpatient infections with patients on methotrexate and TNF inhibitors. Disease activity, a history of previous infection and medications are important factors that must be accounted for in studies of infection in patients with RA.
References
Footnotes
-
Funding The study was supported in part by funding from Amgen. Amgen had no role in the study design, data collection, data analysis, or writing of the manuscript.
-
Competing interests GR has a research contract with CORRONA. JRC receives salary support from NIH (AR053351). He is a consultant for Amgen, Centocor, CORRONA, Pfizer, Roche/Genentech, UCB and received research support from Amgen, Centocor, CORRONA, Roche/Genentech. He also serves as the director of ACIP, a clinical trials unit at UAB that studies rheumatological diseases. JMK receives research support from Amgen, Abbott, Centocor, BMS, Genentech, HGS, Pfizer, Roche and UCB as well as honoraria from Abbott, Centocor, BMS, Roche and Genentech. JDG receives salary support from research grants from the NIH (K23AR054412), the Arthritis Foundation and the Arthritis National Research Foundation. He serves as Chief Scientific Officer for CORRONA and has served on advisory boards for Centocor, Genentech and UCB. VS is a consultant for Abbott, Alder, Allergan, Almirall, Amgen, AstraZeneca, BiogenIdec, CBio, CanFite, Centocor, Chelsea, Crescendo, Cypress Biosciences, Eurodiagnostica, Fibrogen, Forest Laboratories, Genentech, GlaxoSmithKline, HGS, Idera, Incyte, Jazz Pharmaceuticals, Lexicon Genetics, Lilly, Logical Therapeutics, Lux Biosciences, Medimmune, MerckSerono, Novartis, NovoNordisk, Nicox, Nuon, Ono Pharmaceuticals, Pfizer, Rigel, Roche, Sanofi-Aventis, Savient, Schering Plough, SKK, UCB and Xdx. She serves on advisory boards for Abbott, Amgen, BiogenIdec, BMS, CanFite, Centocor, Chelsea, Crescendo, Cypress, Eurodiagnostica, Fibrogen, Forest, Genentech, GSK, HGS, Idera, Incyte, Jazz, Lilly, Nicox, Novartis, NovoNordisk, Pfizer, Rigel, Roche, Savient, Schering Plough and UCB. DEF receives funding from Abbott, Actelion, Amgen, BMS, BiogenIdec, Centocor, Corrona, Genentech, Gilead, GSK, Human Genome sciences, Merck, NIH, Nitec, Novartis, Roche, UCB, Wyeth and Xoma. He also serves as Director of Publications for CORRONA. KA delares no competing interests.
-
Ethics approval Approval from the institutional review boards of each site was obtained before the start of the study.
-
Provenance and peer review Not commissioned; externally peer reviewed.