
Abstract
BNT162b2 (Comirnaty®; BioNTech and Pfizer) is a lipid nanoparticle-formulated, nucleoside-modified mRNA vaccine for the prevention of the novel coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. BNT162b2 encodes the SARS-CoV-2 spike protein, the expression of which elicits immune responses against the antigen in recipients. In early December 2020, BNT162b2 received a temporary emergency use authorization (EUA) in the UK and, subsequently, a series of approvals or authorizations for emergency use in Bahrain, Canada, Mexico, Saudi Arabia and the USA. Soon after, BNT162b2 received conditional marketing authorizations in Switzerland (19 December 2020) and the EU (21 December 2020) for active immunization to prevent COVID-19 caused by SARS-CoV-2 in individuals 16 years of age and older. BNT162b2 is administered intramuscularly in a two-dose regimen. This article summarizes the milestones in the development of BNT162b2 leading to these first approvals for the prevention of COVID-19.
Similar content being viewed by others


Digital Features for this AdisInsight Report can be found at https://doi.org/10.6084/m9.figshare.13557800. |
A nucleoside-modified mRNA vaccine has been developed by BioNTech and Pfizer for the prevention of COVID-19 |
Received its first emergency use authorization on 2 December 2020 in the United Kingdom |
Received its first conditional approval on 19 December 2020 in Switzerland |
Approved for active immunization to prevent COVID-19 caused by the SARS-CoV-2 virus in people aged 16 and over |
1 Introduction
BNT162b2 (Comirnaty®), a nucleoside-modified mRNA vaccine, has been developed by BioNTech and Pfizer for the prevention of coronavirus disease 2019 (COVID-19), the causative agent of which is the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The COVID-19 pandemic has necessitated an unprecedented acceleration of the traditionally lengthy vaccine development process [1, 2]. Rapid response genetic platforms have facilitated rapid vaccine development [3]. Gene-based vaccines (which include, among others, mRNA vaccines and DNA vaccines) carry genetic instructions for the production of an antigen by the cells of the vaccine recipient. For coronavirus vaccines, the target antigen is the surface spike protein, which is used by the virus to bind and fuse with host cells [3]. BNT162b2 consists of nucleoside-modified mRNA encoding the viral spike glycoprotein of SARS-CoV-2, encapsulated in lipid nanoparticles [4]. BNT162b2 was developed through BioNTech’s Project Lightspeed, which brought mRNA vaccine candidates from concept to clinical development in < 3 months [5]. Phase I/II clinical trials of vaccine candidates including BNT162b2 were initiated in April 2020.

Key milestones in the development of the BNT162b2 mRNA COVID-19 vaccine. WHO World Heath Organisation
On 2 December 2020, BNT162b2 received a temporary emergency use authorization (EUA) in the United Kingdom based on a rolling submission which included phase III data from a multinational clinical trial (NCT04368728) [6]. This initial authorization was followed by a rapid succession of authorizations or approvals for emergency use of BNT162b2 in several countries, with Bahrain, Canada, Mexico, Saudi Arabia and the USA being among the earliest (all prior to 14 December 2020) [7,8,9]. On 19 December 2020, BNT162b2 received a conditional marketing authorization in Switzerland for active immunization to prevent COVID-19 caused by SARS-CoV-2 in people aged 16 and over [10,11,12] and on 21 December, BNT162b2 received a conditional marketing authorization in the EU for use in the same indication [13]. The efficacy and safety of BNT162b2 have not yet been established in children < 16 years of age [4, 12]. On 31 December 2020, BNT162b2 was listed for emergency use by the World Health Organisation, representing the first COVID-19 vaccine to receive emergency validation via this pathway [14]. On 14 February 2021, BNT162b2 became the first COVID-19 vaccine to be granted Special Approval for Emergency in Japan [15].
BNT162b2 is available in a multiuse vial which requires cold storage (posing a logistical challenge for the distribution of the vaccine [16]) and must be thawed and diluted before use [4, 12]. Each vial contains six 30 µg doses after dilution [4]. BNT162b2 is administered intramuscularly (ideally into the deltoid muscle) as a course of two 30 µg doses, with a recommended dose interval of 21 days. Full protection against COVID-19 may not be achieved until 7 days after administration of the second dose [4]. As is the case with other vaccines, BNT162b2 may not protect every recipient [4, 12].
The safety of BNT162b2 continues to be monitored, along with the duration of protection against COVID-19 provided by the vaccine. In addition, the safety and immunogenicity of BNT162b2 in specific populations (including pregnant women and Japanese and Chinese individuals) are being evaluated in ongoing clinical trials.
1.1 Company Agreements
In March 2020, BioNTech and Pfizer agreed to co-develop and distribute a potential mRNA-based vaccine for the prevention of COVID-19 [17]. Under the collaboration terms, BioNTech would receive an upfront payment from Pfizer and be eligible to also receive future milestone payments [18]. Development costs would be shared equally between the two companies. BioNTech and its partners were to provide the vaccine candidates for clinical trials from its European GMP-certified mRNA manufacturing facilities. Together, BioNTech and Pfizer will commercialize the approved vaccine worldwide (excluding China) and scale-up manufacturing capacity for global supply [18]. This collaboration built upon their 2018 agreement to co-develop mRNA-based vaccines for influenza [17]. In July 2020, Pfizer and BioNTech announced an agreement with the US government to provide the USA with 100 million doses of BNT162 upon regulatory approval or EUA [19]. The US government would pay the companies US $1.95 billion for these initial doses and would be able to acquire up to 500 million additional doses [19]. As of November 2020, BioNTech and Pfizer have announced commercial supply agreements for 2020 and 2021 with numerous countries, including Canada, Japan, the UK, the USA and those of the EU (subject to clinical success and regulatory approval of the vaccine) [20]. These total more than 570 million doses, including options to purchase an additional 600 million doses [20]. BioNTech and Pfizer expect to manufacture approximately two billion doses in 2021, based on supply projections [21].

Mechanism of action of BNT162b2 following intramuscular administration
BioNTech and Shanghai Fosun Pharma entered into a research and development agreement in March 2020 [22]. Under the terms of this agreement, the companies would jointly develop BNT162 in China, with BioNTech and its partner Polymun supplying the vaccine for clinical trials from European GMP manufacturing facilities. Fosun Pharma would make an upfront payment to BioNTech and an equity investment for shares in BioNTech, as well as potential future investment and milestone payments. Following regulatory approval, Fosun Pharma will be responsible for commercializing the vaccine in China. Future gross profits from sales of the vaccine in China will be shared between the two companies [22]. In August 2020, BioNTech and Fosun Pharma announced that they intend to collaborate to supply 10 million doses of their BNT162 vaccine to Hong King and Macao (dependent upon clinical success and regulatory approval) [23]. The companies have also recently (December 2020) reported an agreement to supply an initial 100 million doses to Mainland China in 2021 [24].
2 Scientific Summary
2.1 Mechanism of Action
BNT162b2 is comprised of nucleoside-modified mRNA formulated in lipid nanoparticles [4]. The mRNA encodes the membrane-anchored, full-length SARS-CoV-19 spike protein and contains mutations which stabilize the spike protein in an antigenically preferred, prefusion conformation [4, 25]. The lipid nanoparticles protect the non-replicating RNA from degradation and allow it to be delivered into host cells after intramuscular injection. Once inside host cells, the mRNA is translated into SARS-CoV-2 spike protein, which is expressed on the surface of the host cells. The transient expression of this spike antigen induces neutralizing antibody and cellular immune responses against it, which may confer protection against COVID-19 [4, 25].
2.2 Immunogenicity
BNT162b2 induced strong antibody responses in healthy adults aged 19–55 years in a non-randomized, open-label phase I/II trial (NCT04380701) conducted in Germany [26]. Patients were assigned to receive two doses of BNT162b2 1 µg, 10 µg, 20 µg or 30 µg administered 21 days apart (n = 12 per dose cohort). In all dose groups, geometric mean concentrations (GMCs) of spike protein-binding immunoglobulin G (IgG) were increased at 21 days after the first dose, with a strong booster response observed at 7 days after the second dose. While spike protein-binding antibody GMCs decreased between 7 and 63 days after the second dose, they remained considerably higher than those in sera from SARS-CoV-2 convalescent patients. SARS-CoV-2 50% neutralizing geometric mean titres (GMTs) were substantially increased by 7 days after the second dose of BNT162b2 10–30 µg. They then decreased somewhat before stabilizing at around 21 days after the second dose (with follow-up until 63 days after the second dose). When a panel of 19 SARS-CoV-19 spike protein variants were evaluated as targets in pseudovirus neutralization assays, BNT162b2 immune sera demonstrated neutralizing responses against all strains. BNT162b2 elicited a robust expansion of SARS-CoV-19 spike protein-specific CD4+ and CD8+ T cells in the majority of vaccinated participants [26].
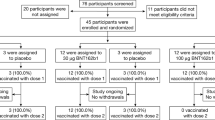
SARS-CoV-2-neutralizing GMTs elicited by BNT162b2 were similar to or higher than those elicited by natural SARS-CoV-2 infection in the randomized, placebo-controlled, observer-blinded, phase I dose-escalation component of the NCT04368728 trial conducted in in healthy adults in the USA (n = 195 randomized) [27]. This phase I component included participants in two age groups (18–55 years and 65–85 years) who received two doses of BNT162b2 or BNT162b1 at a dose level of 10 µg, 20 µg or 30 µg, or placebo, administered 21 days apart (BNT162b1 100 µg was also assessed in the study, but second doses were not administered due to reactogenicity results). As a benchmark, convalescent serum samples were obtained from donors aged 18–83 years who had recovered from SARS-CoV-2 infection or COVID-19. With BNT162b2 30 µg and BNT162b1 30 µg, the 50% neutralizing GMTs at 7 and 14 days after the second dose were 1.7–4.6 times the GMT of the convalescent serum panel in younger adults (aged 18–55 years) and 1.1–2.2 times the GMT of the convalescent serum panel in older adults (aged 65–85 years). BNT162b2 and BNT162b1 elicited comparable immune responses. In both younger and older adults, antigen-binding IgG and virus-neutralizing responses to vaccination (BNT162b2 or BNT162b1 10–30 µg) were augmented by the administration of the second dose, with neutralization titers (obtained prior to the first dose, 21 days after the first dose, and 7 and 14 days after the second dose) being highest at 7 or 14 days after this dose. As is typical with vaccines, antigen-binding IgG and virus-neutralizing responses were generally lower in the older participant group than in the younger group. In each vaccine group, there were 10–12 valid results per assay from samples that could be evaluated at each time point. Immunogenicity results in conjunction with safety data supported the selection of BNT162b2 30 µg for evaluation in the multinational phase II/II component of the trial [27].
Consistent with the breadth of neutralizing response demonstrated against SARS-CoV-2 spike protein variants in NCT04380701[26], BNT162b2 vaccine-elicited sera was recently shown to neutralize engineered SARS-CoV-2 viruses containing key spike mutations (including N501Y) from the newly emerged, rapidly spreading United Kingdom and South African variants [28, 29].
Features and properties of BNT162b2
Alternative names | Tozinameran; BNT 162; BNT 162b2; Bnt-162b2; COMIRNATY; PF-07302048; Pfizer-BioNTech vaccine |
Class | RNA vaccines; viral vaccines |
Mechanism of action | Immunostimulant |
Route of administration | Intramuscular injection |
Adverse events | |
Very common (≥ 1/10) | Injection site pain, fatigue, headache, myalgia, chills, arthralgia, pyrexia, injection site swelling |
Common (≥ 1/100 to < 1/10) | Injection site redness, nausea |
Uncommon (≥ 1/1000 to < 1/100) | Malaise, lymphadenopathy, injection site pruritis, pain in extremity, insomnia |
ATC codes | |
WHO ATC code | JO7B-X (other viral vaccines) |
EphMRA ATC code | J7E9 (all other viral vaccines) |
2.3 Protective Efficacy
BNT162b2 was 95.0% effective (95% CI 90.3–97.6; > 0.9999 posterior probability of true vaccine efficacy being > 30%) in preventing COVID-19 in participants who had no evidence of prior or existing SARS-CoV-2 infection (i.e. no serological or virological evidence of SARS-CoV-2 infection up to 7 days after the second dose) [first primary efficacy endpoint] in the phase II/III component of the pivotal, randomized, placebo-controlled, observer-blinded, global phase I/II/III efficacy trial (NCT04368728); 8 cases of COVID-19 with onset ≥ 7 days after the second dose occurred in BNT162b2 recipients, while 162 cases occurred in placebo recipients [30]. In an analysis including participants with and without evidence of prior SARS-CoV-2 infection, the efficacy of BNT162b2 was 94.6% (95% CI 89.9–97.3; > 0.9999 posterior probability of true vaccine efficacy being > 30%) [second primary efficacy endpoint]; there were 9 cases of COVID-19 with onset ≥ 7 days after the second dose in BNT162b2 recipients, compared with 169 cases in placebo recipients. The efficacy of BNT162b2 was generally consistent across subgroups based on age, sex, race, ethnicity, obesity and pre-existing conditions (lower limit of 95% CI for efficacy > 30% for all subgroups with > 10 cases of COVID-19). In participants without evidence of prior or existing SARS-CoV-2 infection, the efficacy of BNT162b2 was 93.7–100% in subgroups of patients aged 16–55 years, > 55 years, ≥ 65 years and ≥ 75 years. In a separate analysis in participants with hypertension, the efficacy of BNT162b2 was similar to that in the overall population (vaccine efficacy 94.6%; 95% CI 68.7–99.9) [30].
The cumulative incidence of COVID-19 cases in the BNT162b2 group and placebo group began to diverge 12 days after the first dose, suggesting an early onset of partial protection [30]. Between doses one and two, BNT162b2 was 52.4% effective (95% CI 29.5–68.4) in preventing COVID-19, with 39 cases observed in BNT162b2 recipients and 82 cases in placebo recipients. Between the administration of dose two and 7 days after dose two, BNT162b2 was 90.5% effective (95% CI 61.0–98.9) in preventing COVID-19, with cases occurring in two BNT162b2 recipients and 21 placebo recipients. With respect to the occurrence of severe COVID-19, cases occurred in one BNT162b2 recipient and nine placebo recipients after the first dose (vaccine efficacy 88.9%; 95% CI 20.1–99.7) [30].
The phase II/III component of the pivotal trial evaluated vaccine efficacy and safety in adults and adolescents ≥ 16 years of age who were healthy or had stable chronic medical conditions (including, but not limited to, hepatitis B virus infection, hepatitis C virus infection or human immunodeficiency virus) [30]. Those with a medical history of COVID-19, treated with immunosuppressive therapy or diagnosed with an immunocompromising condition were among the excluded. Enrolled participants were randomized to receive two 30 µg doses of either BNT162b2 or placebo, administered 21 days apart, at study sites in the USA, Argentina, Brazil, South Africa, Germany and Turkey. Analyses of the first and second primary efficacy endpoints included 36,523 participants (18,198 BNT162b2 recipients and 18,325 placebo recipients) and 40,137 participants (19,965 and 20,172) respectively [30].
Key clinical trials of BNT162b2 for the prevention of COVID-19 (sponsored by BioNTech)
Vaccine(s) | Phase | Status | Location(s) | Identifier |
|---|---|---|---|---|
BNT162b2, BNT162b1, placebo | I/II/III | Active, not recruiting | Multinational | NCT04368728; C4591001; 2020-002641-42 |
BNT162b2 | III | Not yet recruiting | US- and EU-manufactured batches | NCT04713553; C4591017 |
BNT162b2, BNT162a1, BNT162b1, BNT162c2 | I/II | Recruiting | Germany | NCT04380701; BNT162-01; 2020-001038-36; U1111-1249-4220 |
BNT162b2, placebo | I/II | Active, not recruiting | Japan | NCT04588480 |
BNT162b2, placebo | II | Recruiting | China | NCT04649021; BNT162-06 |
2.4 Adverse Events
BNT162b2 administered as two 30 µg doses 21 days apart was generally well tolerated in the pivotal phase I/II/III trial [27, 30]. In the phase II/III component of the trial (n = 21,621 and 21,631 treated with at least one dose of BNT162b2 and placebo, respectively, with any duration of follow-up; 18,860 and 18,846 participants in the respective groups had a median of ≥ 2 months of safety data after the second dose, 42% of whom were > 55 years of age), adverse events (AEs) were reported in 27% of BNT162b2 recipients versus 12% of placebo recipients while related AEs were reported in 21% versus 5% [30]. These group differences are largely attributed to transient reactogenicity events, which were more common with BNT162b2 than placebo (see below). Few BNT162b2 or placebo recipients experienced severe AEs (1.1% vs 0.6%), serious AEs (0.6% vs 0.5%) or AEs that lead to withdrawal from the trial (0.2% vs 0.1%). Related serious AEs occurred in four BNT162b2 recipients (right axillary lymphadenopathy; right leg paresthesia; shoulder injury related to vaccine administration; paroxysmal ventricular arrhythmia). Deaths, none of which were considered to be related to BNT162b2 or placebo, occurred in two BNT162b2 recipients and four placebo recipients [30].
In a subset of patients from the pivotal trial (i.e. the reactogenicity subset; n = 8183), data on local and systemic reactions were collected using electronic diaries for 7 days after each dose [30]. With respect to solicited local events, injection site pain was the most common, reported in 83% and 78% of younger BNT162b2 recipients (aged 16–55 years) after doses one and two (vs 14% and 12% of younger placebo recipients). Injection site pain was somewhat less common in older BNT162b2 recipients (aged > 55 years), occurring in 71% and 66% after doses one and two (vs 9% and 8% of older placebo recipients). Injection site swelling was reported in 6% of younger BNT162b2 recipients after each dose (compared with 0% of younger placebo recipients), while the respective rates in older BNT162b2 and placebo recipients were 7% and 1% after each dose. Injection site redness was reported in 5% and 6% of younger BNT162b2 recipients after doses one and two (vs 1% of placebo recipients after each dose), while the respective rates in older BNT162b2 recipients were 5% and 7% (vs 1%). Local reactions were generally of mild to moderate severity, resolving within 1–2 days; there were no grade 4 local reactions [30].
The systemic events most commonly reported in younger BNT162b2 recipients (≥ 10% after either dose) were fatigue (47% and 59% after doses one and two vs 33% and 23% with placebo), headache (42% and 52% vs 34% and 24%), muscle pain (21% and 37% vs 11% and 8%), chills (14% and 35% vs 6% and 4%), joint pain (11% and 22% vs 6% and 5%), diarrhoea (11% and 10% vs 12% and 8%) and fever (4% and 16% vs 1% and 0%) [30]. Systemic events were generally less common in older BNT162b2 recipients. Those occurring in ≥ 10% of older BNT162b2 recipients (after either dose) were fatigue (34% and 51% after doses one and two vs 23% and 17% with placebo), headache (25% and 39% vs 18% and 14%), muscle pain (14% and 29% vs 8 and 5%), chills (6% and 23% vs 3% and 3%), joint pain (9% and 19% vs 6% and 4%) and fever (1% and 11% vs 0% and 0%). Most systemic events were mild to moderate severity; severe systemic events occurred in < 2% of BNT162b2 recipients after each dose, with the exception of fatigue and headache after the second dose (occurring in 4% and 2%, respectively). They were typically observed in the first 1–2 days after the vaccine, resolving soon after [30].
Events of anaphylaxis have been reported with BNT162b2 [4, 31]. Vaccine Adverse Event Reporting System monitoring in the USA (14–23 December 2020) detected 21 cases of anaphylaxis after 1,893,360 first doses of BNT162b2 were administered (a rate of 11.1 cases per million doses) [31]. The majority of cases occurred within 15 min of administration (71%; range 2–150 min), in females (90%) and in individuals with a documented history of allergies or allergic reactions (81%). The median age of patients with anaphylaxis was 40 years (range 27–60 years). In cases where follow-up information was available (95%), the patient had recovered or been discharged from hospital [31]. Following administration of BNT162b2, close observation is recommended for ≥ 15 min and appropriate medical treatment needs to be readily available in case of an anaphylactic reaction [4]. Individuals who experience anaphylaxis to the first dose of BNT162b2 should not receive a second dose [4].
Due to limited data, the use of BNT162b2 during pregnancy should only be considered if the potential benefits are deemed to outweigh any potential risks for the mother and foetus [4]. It is unknown whether BNT162b2 is present in human breast milk [4].
2.5 Ongoing Clinical Trials
The pivotal phase I/II/III trial (which has enrolled participants ≥ 12 years of age) is ongoing, with safety monitoring to continue for 2 years after administration of the second BNT162b2 dose [30]. Also underway is a randomized, placebo-controlled, phase I/II trial (NCT04588480) evaluating the safety, tolerability and immunogenicity of BNT162b2 in Japanese adults. In Germany, the safety and immunogenicity of four BNT162 vaccines (including BNT162b2) are being assessed in a multicenter, phase I/II dose-escalation study (NCT04380701; currently recruiting). A randomized, placebo-controlled, phase II trial (NCT04649021) evaluating the safety and immunogenicity of BNT162b2 has recently started to recruit healthy adults in China.
While yet to begin recruitment, a randomized, observer-blind phase III trial (NCT04713553) in healthy individuals aged 18–55 years will evaluate the consistency of five BNT162b2 manufacturing production lots in the USA and EU with respect to vaccine safety, tolerability and immunogenicity. A randomized, placebo-controlled, observer-blind, phase II/III trial (NCT04754594) will evaluate the safety, tolerability, and immunogenicity of BNT162b2 in healthy pregnant women (aged ≥ 18 years) administered the vaccine at 24 to 34 weeks' gestation.
3 Current Status
The BNT162b2 mRNA COVID-19 vaccine received its first conditional approval on 19 December 2020 in Switzerland for active immunization to prevent COVID-19 caused by the SARS-CoV-2 virus in people aged 16 and over. BNT162b2 has subsequently received a conditional approval in the EU.
References
Krammer F. SARS-CoV-2 vaccines in development. Nature. 2020;586(7830):516–27.
Rego GNA, Nucci MP, Alves AH, et al. Current clinical trials protocols and the global effort for immunization against SARS-CoV-2. Vaccines. 2020;8(3):1–44.
Abbasi J. COVID-19 and mRNA vaccines - first large test for a new approach. JAMA. 2020;324(12):1125–7.
European Medicines Agency. Covid-19 mRNA vaccine (Comirnaty): EU summary of product characteristics. 2020. http://ec.europa.eu. Accessed 11 Feb 2021.
BioNTech. Aiming to address the global coronavirus pandemic: Project Lightspeed. 2020. https://biontech.de. Accessed 11 Feb 2021.
Pfizer. Pfizer and BioNTech achieve first authorization in the world for a vaccine to combat COVID-19 [media release]. 2 Dec 2020. http://www.pfizer.com.
BioNTech. Pfizer and BioNTech provide data from German phase 1/2 study further characterizing immune response following immunization with lead COVID-19 vaccine candidate BNT162b2 [media release]. 14 Dec 2020. http://www.biontech.de.
Government of Canada. Health Canada authorizes first COVID-19 vaccine [media release]. 9 Dec 2020. http://www.canada.ca.
US Food and Drug Administration. FDA takes key action in fight against COVID-19 by issuing emergency use authorization for first COVID-19 vaccine [media release]. 11 Dec 2020. http://www.fda.gov.
Pfizer. Pfizer and BioNTech receive Conditional Marketing Authorization by Swissmedic for COVID-19 vaccine [media release]. 19 Dec 2020. http://www.pfizer.com.
Swissmedic. Swissmedic grants authorisation for the first COVID-19 vaccine in Switzerland [media release]. 19 Dec 2020. http://www.swissmedic.ch.
Swissmedic. Comirnaty®: Fachinformation. 2020. http://www.swissmedicinfo.ch. Accessed 11 Feb 2021.
Pfizer. Pfizer and BioNTech receive authorization in the European Union for COVID-19 vaccine [media release]. 21 Dec 2020. http://www.pfizer.com.
World Health Organisation. WHO issues its first emergency use validation for a COVID-19 vaccine and emphasizes need for equitable global access [media release]. 31 Jan 2020. http://www.who.int.
Pharmaceuticals and Medical Devices Agency. Special Approval for Emergency on first COVID-19 vaccine in Japan [media release]. 16 Feb 2021. http://www.pmda.go.jp.
Burki T. Equitable distribution of COVID-19 vaccines. Lancet. 2021;21(1):P33–4.
Pfizer. Pfizer and BioNTech to co-develop potential COVID-19 vaccine [media release]. 17 Mar 2020. http://www.pfizer.com.
Pfizer, BioNTech. Pfizer and BioNTech announce further details on collaboration to accelerate global COVID-19 vaccine development [media release]. 9 Apr 2020. http://www.pfizer.com.
Pfizer. Pfizer update on our U.S. COVID-19 vaccine candidate distribution preparedness [media release]. 16 Nov 2020. http://www.pfizer.com.
BioNTech. BioNTech announces third quarter 2020 financial results and corporate progress [media release]. 10 Nov 2020. http://www.biontech.de.
Pfizer. Pfizer and BioNTech to supply the European Union with 200 million additional doses of COMIRNATY® [media release]. 17 Feb 2021. http://www.pfizer.com.
BioNTech, Fosun Pharma. BioNTech and Fosun Pharma form COVID-19 vaccine strategic alliance in China [media release]. 16 Mar 2020. http://www.biontech.de.
BioNTech, Fosun Pharma. BioNTech and Fosun Pharma to potentially supply 10 million doses of BioNTech's BNT162 mRNA-based vaccine candidate against SARS-CoV-2 to Hong Kong SAR and Macao SAR [media release]. 27 Aug 2020. http://www.biontech.de.
BioNTech. BioNTech and Fosun Pharma to supply China with mRNA-based COVID-19 vaccine [media release]. 16 Dec 2020. http://www.biontech.de.
European Medicines Agency. Comirnaty: CHMP public assessment report. 2020. http://www.ema.europa.eu. Accessed 11 Feb 2021.
Sahin U, Muik A, Vogler I, et al. BNT162b2 induces SARS-CoV-2-neutralising antibodies and T cells in humans. medRxiv. 2020:2020.12.09.20245175.
Walsh EE, Frenck RW Jr, Falsey AR, et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N Engl J Med. 2020;14:14.
BioNTech. An in vitro study shows Pfizer-BioNTech COVID-19 vaccine elicits antibodies that neutralize SARS-CoV-2 with a mutation associated with rapid transmission [media release]. 8 Jan 2021. http://www.biontech.de.
Xie X, Liu Y, Liu J, et al. Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K, and N501Y variants by BNT162b2 vaccine-elicited sera. medRxiv. 2021. https://doi.org/10.1101/2021.01.24.427991.
Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;10:10.
CDC COVID-19 Response Team, Food and Drug Administration. Allergic reactions including anaphylaxis after receipt of the first dose of Pfizer-BioNTech COVID-19 vaccine—United States, December 14–23, 2020. MMWR Morb Mortal Wkly Rep. 2021;70(2):46–51.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The preparation of this review was not supported by any external funding.
Authorship and Conflict of interest
During the peer review process the manufacturer of the agent under review was offered an opportunity to comment on the article. Changes resulting from any comments received were made by the authors on the basis of scientific completeness and accuracy. Yvette Lamb is a salaried employee of Adis International Ltd/Springer Nature, and declares no relevant conflicts of interest. All authors contributed to the review and are responsible for the article content.
Ethics approval, Consent to participate, Consent to publish, Availability of data and material, Code availability
Not applicable.
Additional information
This profile has been extracted and modified from the AdisInsight database. AdisInsight tracks drug development worldwide through the entire development process, from discovery, through pre-clinical and clinical studies to market launch and beyond.
Rights and permissions
About this article

Cite this article
Lamb, Y.N. BNT162b2 mRNA COVID-19 Vaccine: First Approval. Drugs 81, 495–501 (2021). https://doi.org/10.1007/s40265-021-01480-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-021-01480-7