Article Text

Statistics from Altmetric.com
- respiratory medicine
- lung cancer (oncology)
- cardiovascular medicine
- cancer - see oncology
- pericardial disease
Description
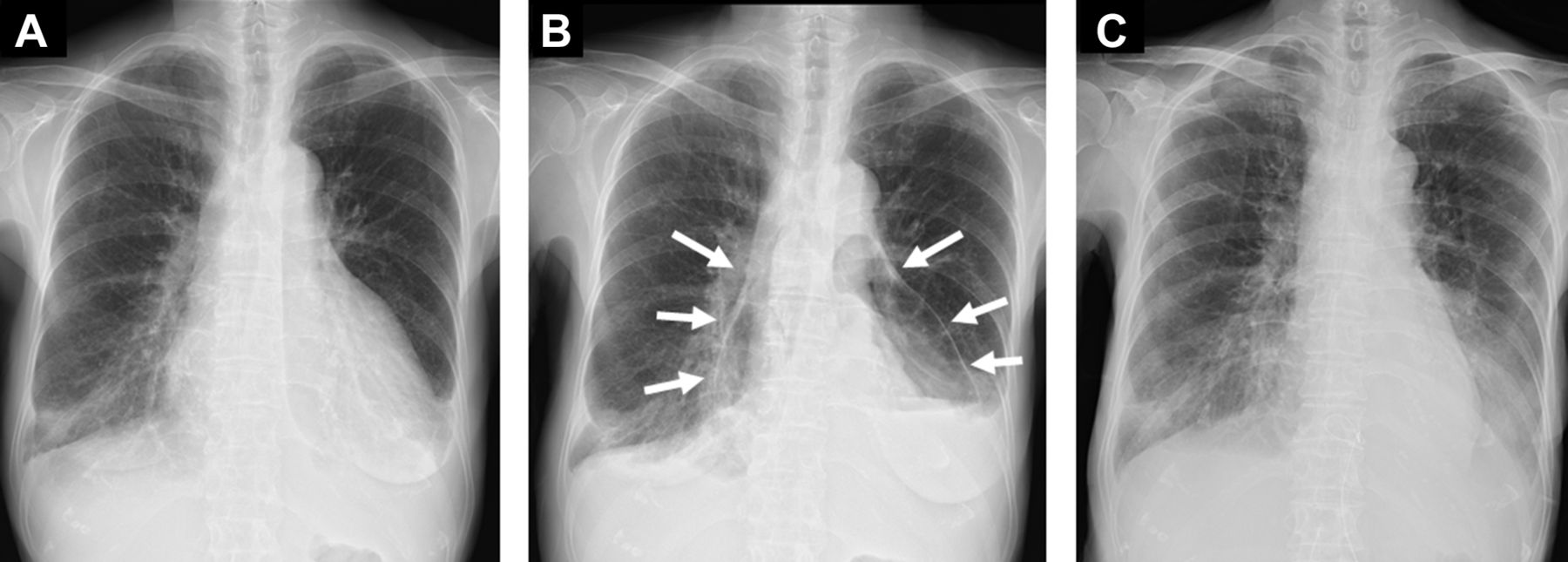
A 74-year-old Japanese woman with no remarkable medical history reported lower extremity oedema for 4 months before visiting our hospital. She presented with breathing difficulty at admission and subsequently reported coughing and paroxysmal nocturnal dyspnoea 1 month prior to admission. Chest radiography revealed cardiac dilation and bilateral pleural effusion. Chest and abdominal CT and PET revealed nodules and enlargement of the right paratracheal lymph node in the right lung, abdominal lymphadenopathy, and pericardial and pleural accumulations of fluid. Adenocarcinoma was detected during pleural effusion examination. The patient was diagnosed with cT2aN3M1b stage IV pulmonary primary adenocarcinoma following a bronchoscopic examination. Cardiac tamponade was suspected based on a systolic blood pressure of 90 mm Hg, pulse of 120 bpm and oxygen saturation of 90% on room air; therefore, a cardiac puncture without continuous suction was performed. Following puncture, the radiolucent pockets representing air appeared on chest radiography in the same location from which the pericardial effusion had been removed (figure 1A,B). Chest CT image showed air fluid level within the pericardial sac (figure 2) and the absence of any fistulous tracts between the pericardium and trachea/airways. Additionally, cytological analysis of the pericardial fluid revealed adenocarcinoma cells. These findings are consistent with pneumopericardium on a background of carcinomatous pericarditis. We found insufficient improvement of hypotension and hypoxia; therefore, we performed cardiac puncture and applied continuous negative pressure. This resulted in an improvement in the pneumopericardium (figure 1C). In addition, real-time PCR, which was performed with paraffin fixed specimens of lung tissue, revealed that the patient carried the EGFR 21 L858R mutation, and erlotinib was prescribed for treatment of the lung adenocarcinoma. Since it is thought that the EGFR tyrosine kinase inhibitor may exhibit high tumour control effect in EGFR positive lung adenocarcinoma and carcinomatous pericarditis, systemic chemotherapy with erlotinib is first performed. We had planned treatment with pericardial adhesion or pericardiotomy, if the pericardial water increased again. Due to adverse events, erlotinib was changed to gefitinib and a cytotoxic anticancer agent was also administered.

Chest radiograph (A) before cardiac puncture; (B) after cardiac puncture, with signs of pneumopericardium (white arrows); (C) and after the application of continuous negative pressure.

{kind=link}
{kind=link}
Chest CT image showing air fluid level caused by pneumopericardium.
However, after about 22 months from the first visit, the patient died as the treatment was not effective. Recurrent pericardial effusion was not observed during treatment, and in the CT scan, 1 month before death.
Pneumopericardium is the accumulation of gas in the pericardial cavity. It is most commonly caused by direct trauma to the pericardial layer surrounding the heart.1 Iatrogenic pneumopericardium as a consequence of pericardiocentesis is rare and mostly results from a leak in the drainage system or formation of communication between the pleura and pericardium.2 In the present case, the pericardium stretched slightly due to carcinomatous pericarditis. Cardiac puncture without continuous suction left air in the pericardium. Cardiac repuncture and application of continuous negative pressure resulted in the improvement of the pneumopericardium. Although pericardiocentesis is rarely associated with serious complications, meticulous procedural technique and postprocedure monitoring including chest radiography are necessary.
Learning points
Pneumopericardium is the accumulation of gas in the pericardial cavity. It is most commonly caused by direct trauma to the pericardial layer surrounding the heart.
Iatrogenic pneumopericardium as a consequence of pericardiocentesis is rare. However, meticulous procedural technique and postprocedure monitoring including chest radiography are necessary.
Footnotes
Contributors TK managed redaction, correction and reconstruction of the manuscript. KM managed the case and redaction and correction of the manuscript. HN assisted with clinical management of the case and correction of the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.