Article Text

Statistics from Altmetric.com
Description
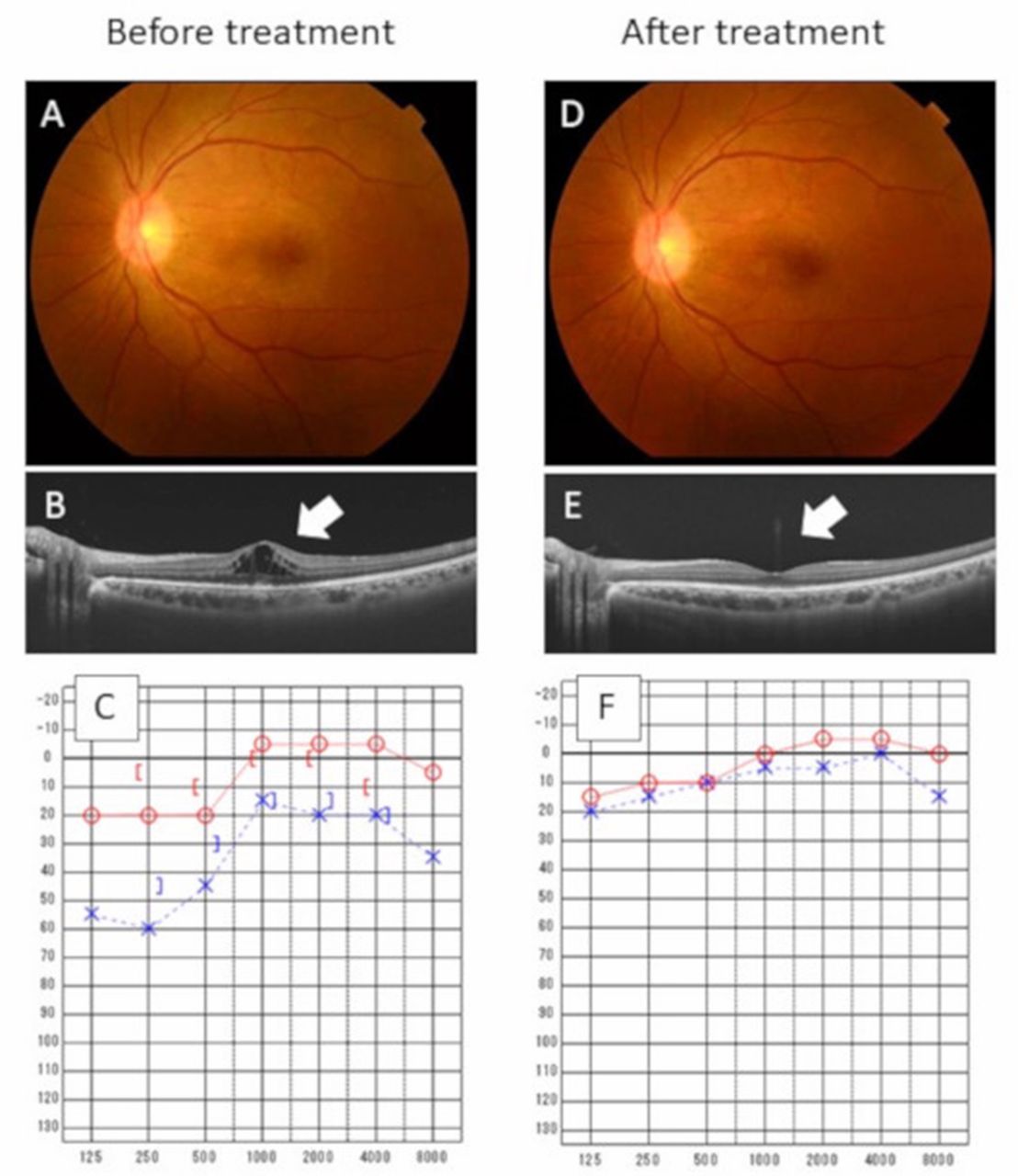
A 42-year-old woman presented to our hospital with a 2-month history of bilateral decreased and blurry vision accompanying mild photophobia. She had had several episodes of unsafe sex and was diagnosed with secondary syphilis 10 months prior. Despite the diagnosis, she did not undergo any treatment for the infection. An ophthalmological examination revealed bilateral macular oedema, suggesting the development of uveitis (figure 1A,B). Laboratory data for complete blood counts and chemistry were unremarkable, but there were elevations of rapid plasma reagin (RPR) test and Treponema pallidum haemagglutination test (TPHA) titres, at 1:32 and 1:5120, respectively, leading to the diagnosis of ocular syphilis. Screening tests for hepatitis B virus, hepatitis C virus and HIV yielded negative findings. Further cerebrospinal fluid examination indicated a complication of neurosyphilis, with a mildly elevated white cell count (0.013×109/L), protein level (49 mg/dL), and positive RPR (1:4) and TPHA (1:320) titres. The patient was scheduled to be hospitalised in order to undergo intravenous treatment. Before admission, the patient suddenly experienced hearing deficit. The Weber test showed lateralisation to the right ear and the Rinne test was positive in the left ear, suggesting a left sensorineural hearing deficit, which was proven by an audiogram (figure 1C). Brain MRI did not show any remarkable findings in her brain. Having been diagnosed with ocular and otosyphilis, we administered aqueous penicillin G (24 million units per day) along with prednisone (0.5 mg/kg). After completing 14 days of antibiotic therapy, the patient was discharged without any complications. Her visual symptoms improved, and macular oedema and loss of ellipsoid zone were dramatically improved (figure 1D,E). The auditory dysfunction resolved as well (figure 1F). After 4 months of treatment, serum titres of RPR decreased to 1:8.
{kind=link}
Fundus photograph, optical coherence tomography and audiogram. White colour appearance observed inside the vascular arcade before treatment (A) disappeared 1 month after treatment (D). Optical coherence tomography showed a decrease in macular oedema and resolution of the loss of ellipsoid zone (B, E; arrow). Auditory function also improved after treatment (C, F).
Syphilis, a classical sexually transmitted infection caused by Treponema pallidum, has globally re-emerged as a silent pathogen, reaching up to more than 4000 cases in 2016 in Japan.1 Although typical manifestations of the disease include genital and dermatological symptoms, the infection potentially causes systemic abnormalities. Neurosyphilis is the representative condition, which commonly occurs at a late stage (more than 1 year) of the infection. Concurrent complications of ocular and auditory dysfunction are considered extremely rare,2 3 although an exact prevalence of such a condition is unknown. Reviewing the patient’s clinical course, she developed the ocular and otosyphilis at almost 1 year after infection with the pathogen. General physicians should recall that syphilis is a possible aetiology of multiple cranial nerve manifestations.
Learning points
Syphilis, a re-emerging silent pathogen, potentially causes various manifestations during the course of infection.
This case highlights the concurrent development of ocular and otosyphilis almost 1 year after infection.
Clinicians should note that syphilis can present in various diverse manifestations.
Acknowledgments
We are grateful to Hiromi Rakugi (Department of General Internal Medicine, Osaka University Hospital) for his advice and warm encouragement.
Footnotes
Contributors All the authors contributed management of the patient and writing of this report. Especially, FN, KM and YO mainly managed the patient. HH mainly wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.