Article Text

Statistics from Altmetric.com
Description
A 38-year-old man presented with intermittent right flank pain, dysuria, passage of turbid urine and low-grade fever for the last 1 year. He revealed a history of right-sided laparoscopic Anderson-Hynes dismembered pyeloplasty with double J (DJ) stenting performed for right pelviureteric junction obstruction 5 years back at other centre. The discharge card given to the patient advised for DJ stent removal, but the patient was lost to follow-up and never underwent DJ removal. His medical history was unremarkable for diabetes, HIV or steroid intake. On physical examination there was tenderness present in right flank on deep palpation. Blood serum chemistries revealed mildly deranged renal function tests (blood urea nitrogen 56 mg/dL; serum creatinine 1.5 mg/dL) with normal random blood sugar (92 mg/dL) and liver function tests. Urine analysis showed 40–50 pus cells/high power field (HPF), 20 red blood cells/HPF and presence of fungal hyphae and spores. Urine culture revealed >105 colony counts of Candida albicans per mL.
On evaluation with kidney, ureter and bladder X-ray there was presence of right DJ stent without encrustation and radiopaque shadow in left renal region (figure 1A). Ultrasonography of abdomen revealed severely dilated right kidney showing multiple hyperechoic rounded lesions (15–25 mm) with a DJ stent in situ and left renal pelvic calculus (21 mm) (figure 1B). Further evaluation with contrast enhanced CT scan of abdomen showed presence of isodense non-enhancing multiple intraluminal filling defects with tiny peripheral calcifications in massively dilated right renal pelvis (suggestive of fungal balls) (figure 2). The patient underwent ureteric stent removal followed by placement of right-sided percutaneous nephrostomy (PCN). It initially drained about 500 mL turbid urine mixed with debris and flakes in first 24 hours followed by minimal output. He received oral fluconazole (400 mg) once daily treatment for 2 weeks with gravity-dependent low-pressure intrapelvic instillation of deoxycholate amphotericin B (10 mg/L of 5% dextrose in water) via PCN. Further evaluation with Tc 99 m renal scan revealed non-functioning right kidney. After proper counselling and consent, he underwent right nephrectomy followed by left percutaneous nephrolithotomy. At 3 months of follow-up, he was doing well with no residual stone or hydronephrosis on ultrasound abdomen on left side.

(A) Kidney, ureter and bladder (KUB) X-ray image showing presence of right double J (DJ) stent without encrustation and radiopaque shadow in left renal region. (B) Ultrasonography image showing severely dilated right kidney with multiple hyperechoic rounded lesions.
{kind=link}
{kind=link}
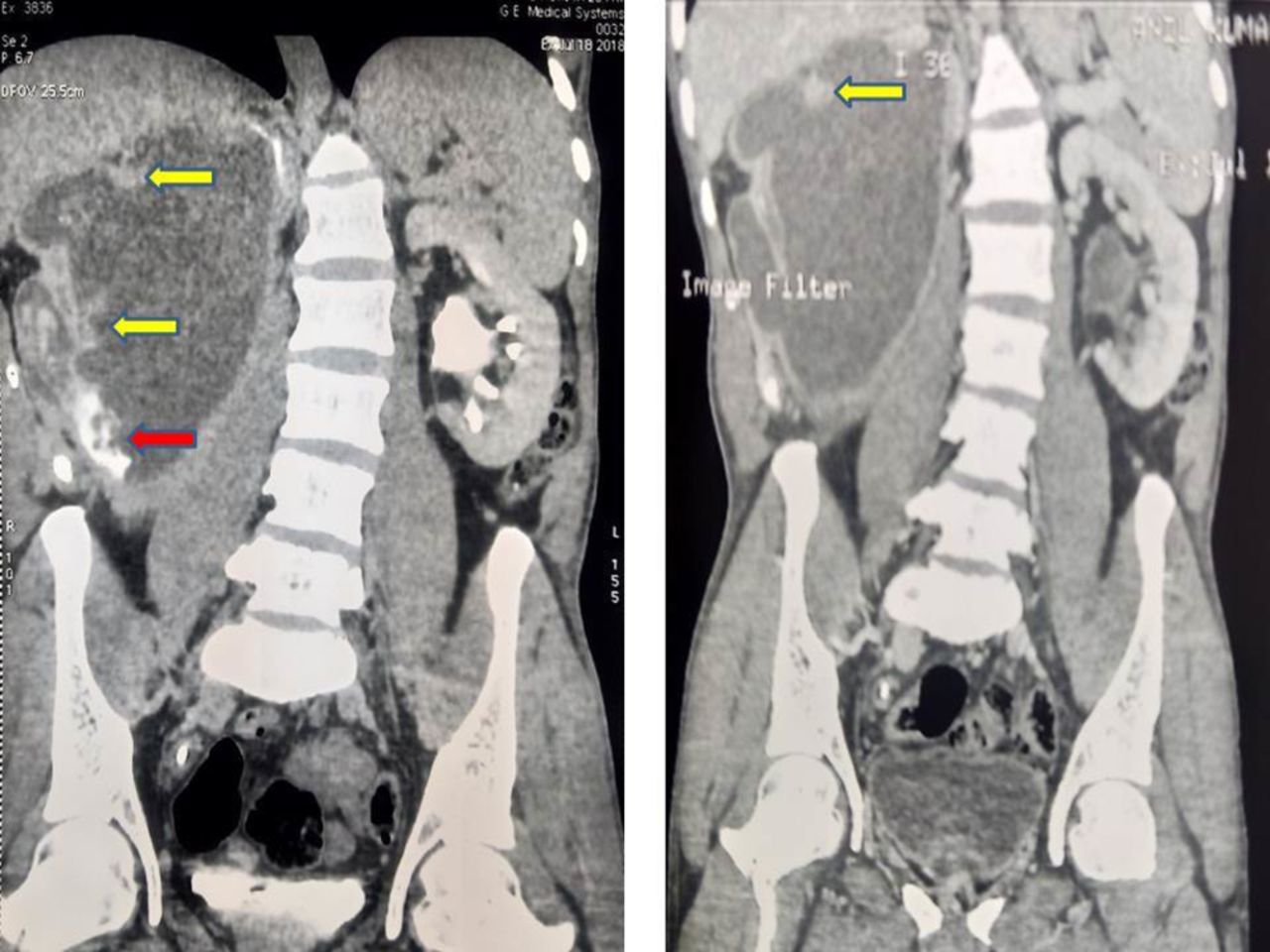
Contrast enhanced CT scan of abdomen showing presence of isodense non-enhancing multiple intraluminal filling defects with tiny peripheral calcifications in massively dilated right renal pelvis (yellow arrow—multiple filling defects near renal pelvic wall, red arrow—filling defects with tiny calcifications).
The fungal infections of upper urinary tract are relatively uncommon entity, and fungal bezoar is particularly rare.1 In literature, only handful cases of renal or ureteric fungal bezoar are reported and mostly in immunocompromised individuals. These fungal bezoars are usually formed by localised clusters of fungal mycelia without adjacent tissue invasion and sometimes it may become large enough to cause obstructive uropathy. The predisposing risk factors include diabetes, prolonged bladder catheterisation or retained foreign body, malignancy and prolonged antibiotic administration.2 Untreated fungal infections can lead to urinary tract obstruction, urosepsis, hydronephrosis and secondary renal damage.3 The preferred treatment of upper tract fungal infections is urinary drainage by a nephrostomy tube or ureteral catheter along with systemic and local antifungal administration and removal of foreign body.3 In the present case, an immunocompetent patient developed upper tract fungal infection (bezoar) as the forgotten DJ stent provided a nidus for fungal growth and proliferation.
Learning points
Fungal bezoar is a rare upper urinary tract infection mostly seen in immunocompromised individuals.
In rare cases, fungal bezoar may develop in immune competent individuals as a complication of forgotten double J stent.
The urinary tract obstruction, urosepsis, hydronephrosis and secondary renal damage are very rare complications of fungaluria.
The preferred treatments of upper tract fungal infections are systemic and local antifungal administration, urinary drainage with percutaneous nephrostomy or ureteric stent and removal of foreign body.
Footnotes
Contributors AS and GG: concept, design, supervision, processing, writing of manuscript and critical analysis. DS: supervision, processing, writing of manuscript and critical analysis. MS: concept, supervision, writing of manuscript and critical analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.