Article Text

Statistics from Altmetric.com
Description
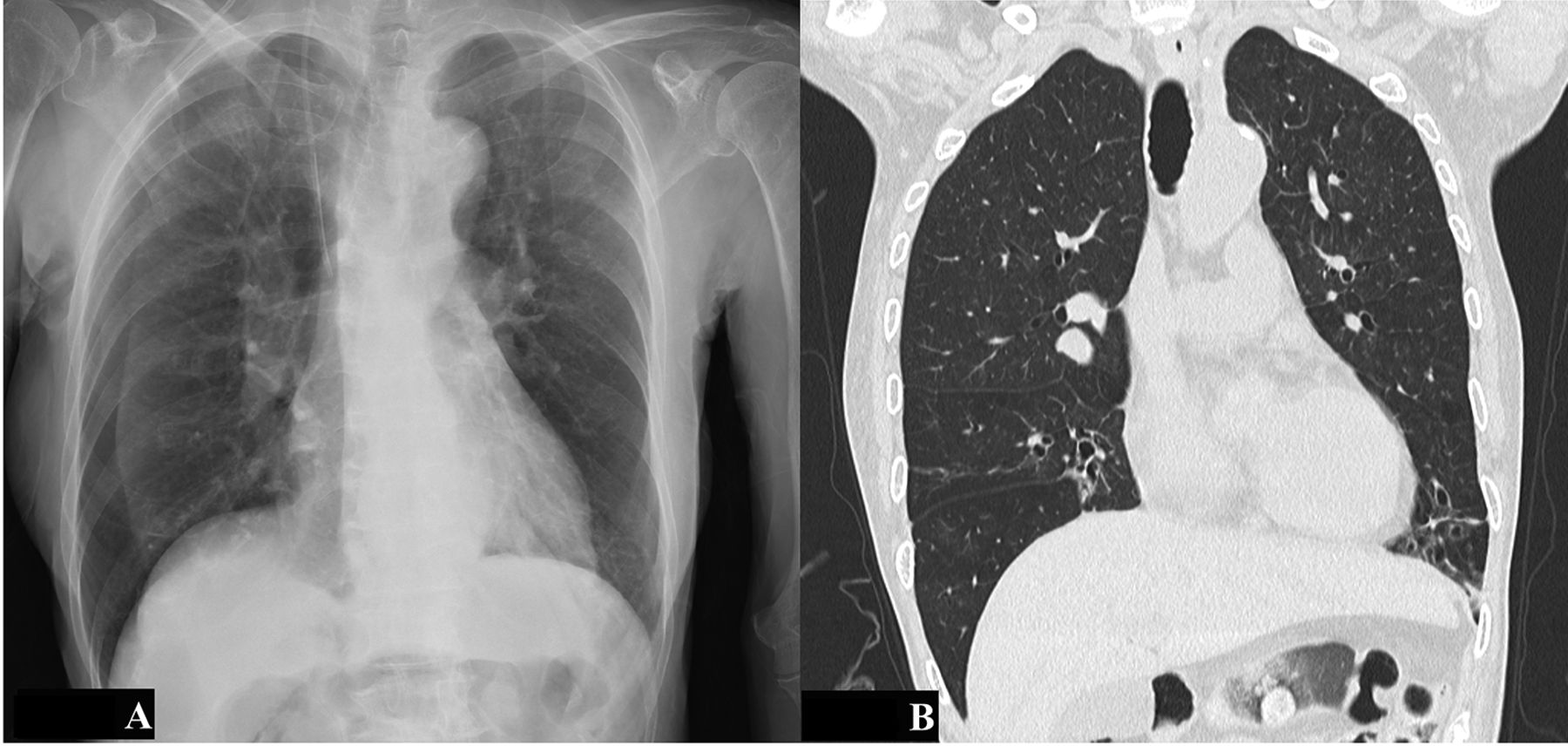
A 79-year-old hospitalised woman underwent central venous catheterisation for high-calorie infusion. Chest radiography to check the position of the catheter showed a curvilinear line at the lateral zone of the right lung (figure 1A). We suspected pneumothorax and performed CT of the chest. However, it revealed the absence of pneumothorax; the curvilinear mimicked pneumothorax was revealed to be a skinfold (figure 1B).

{kind=link}
(A) Initial chest radiograph showed a curvilinear line at the right lateral zone of the right lung. (B) CT of the chest revealed the absence of pneumothorax.
The lateral margin of the skinfold artefact, caused by compression of flaccid back skin against the film, can be sharply outlined by a lucent line.1 This line is an edge enhancement phenomenon at the margin between objects with different contrast or luminance (Mach band effect).2 The area lateral to the skinfold artefact may be perceived darker than the hilar side because of the added density of the skinfold.
The lung marking sign is useful for differentiate pneumothorax from the other conditions, but in the emphysema and bullous disease, the lung marking can be vanished. Poor or no visualisation of normal lung and vascular tissues of the lateral side reinforced the similar appearance of pneumothorax. In a case with hubbly collapse of pneumothorax, the lung marking can be seen beyond the outside of the collapsed lung.3 In some situations, pneumothorax and skinfold might be difficult to differentiate on chest radiography. In those cases, lung ultrasonography or CT facilitators are helpful to make a correct diagnosis.
Patient’s perspective
If my chest X-ray findings have many points to learn, please use it as a study material.
Learning points
Skinfold shadow is a frequent artefact on the anterior-posterior portable chest radiographs of patients in the critical care setting.
Pneumothorax and skinfold might be difficult to differentiate on chest radiography. In those cases, lung ultrasonography or CT facilitators are helpful to make a correct diagnosis.
Acknowledgments
The authors thank Professor Kazumichi Onigata of the Postgraduate Clinical Training Centre at Shimane University Hospital for his careful supervision of young physicians.
Footnotes
Contributors KK cared the patient. TW and YT supervised KK and revised the draft. All contributed in writing and editing and finally approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.