Article Text

Summary
We report a case of calcium pyrophosphate deposition disease (CPPD) with an unusual presentation of severe chondrocalcinosis with atypical large burden deposited in the metacarpophalangeal joints as well as more typical deposition in wrists and knees as demonstrated on plain radiographs. A 77-year-old African-American woman 1-year status post parathyroidectomy for hyperparathyroidism initially presented to the rheumatology clinic to treat suspected rheumatoid arthritis given her pattern of joint involvement but was found to have CPPD. The patient’s history is notable for end-stage renal disease which complicates medical management. This case illustrates radiographic findings of CPPD and explores the challenges of treating CPPD in the setting of comorbid conditions.
- rheumatology
- degenerative joint disease
- gout
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Calcium pyrophosphate deposition disease (CPPD) is often difficult to distinguish from other joint pathologies based on clinical findings alone, which makes it an important disease to consider in the setting of joint pain. The pathogenesis of CPPD has not been fully elucidated but the formation of calcium pyrophosphate dihydrate (CPP) crystals in the pericellular matrix of cartilage has been found to be a primary first step.1 CPPD is classically defined as having three distinct phenotypes including: acute (self-limited synovitis, formerly known as pseudogout), chronic (lasting several months) and asymptomatic CPPD.2 In the chronic form of CPPD, destruction occurs over time resulting in degenerative changes and osteoarthritis of the affected joints. The incidence of CPPD is known to increase with age and may be idiopathic, but known risk factors include a family history of CPPD and known polymorphisms in the ANKH gene (which encodes a transmembrane inorganic pyrophosphate shuttle protein), osteoarthritis (OA), chronic kidney disease (CKD), hyperparathyroidism, hypomagnesaemia and haemochromatosis.3–5 Symptoms may include pain, warmth and swelling of affected joints especially in acute attacks. Acute attacks of CPPD may last for weeks to months.6 However, many cases of CPPD are asymptomatic. CPPD is a systemic disease commonly resulting in a polyarticular pattern. Typical areas affected include joints of the knees, wrists, shoulders or hips.3 7 Any combination of these joints may be involved, and less often, CPPD can be monoarticular. Rarely, CPP crystals will deposit in intervertebral discs.8
Diagnosis of CPPD is confirmed by synovial fluid analysis demonstrating weakly positively birefringent rhomboid crystals in contrast to the negatively birefringent monosodium urate crystals observed in gout.2 In chronic cases, a radiographic hallmark that differentiates CPPD from rheumatoid arthritis (RA) is the presence of chondrocalcinosis on plain film. Most common radiographic findings are found in the triangular cartilage of the carpal bones and menisci of the knee. Rarely, chondrocalcinosis is observed in the metacarpophalangeal (MCP) joints and can mimic RA, deemed pseudo-rheumatism. Patients with chondrocalcinosis in MCP joints can have a three to six times greater likelihood of developing secondary OA.9 10 Treatment options begin with non-steroidal anti-inflammatory drugs and colchicine in the acute setting. Corticosteroid injection or oral therapy may be added depending on the number of joints involved, and varying regimens may be escalated to achieve efficacy. Several novel selective agents that target specific pathways could potentially be effective in CPPD, and therapeutic strategies are reviewed here.2 11
Case presentation
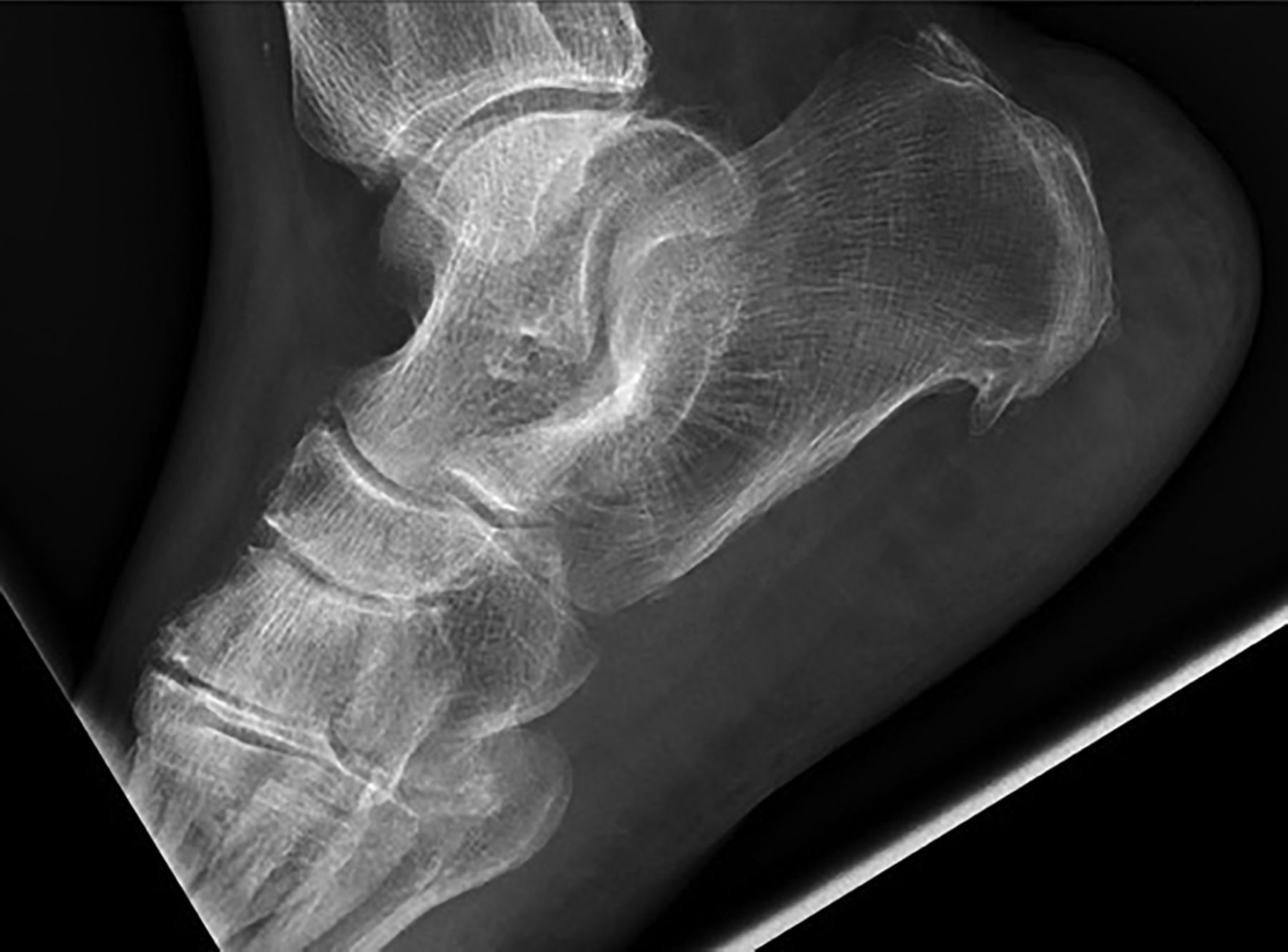
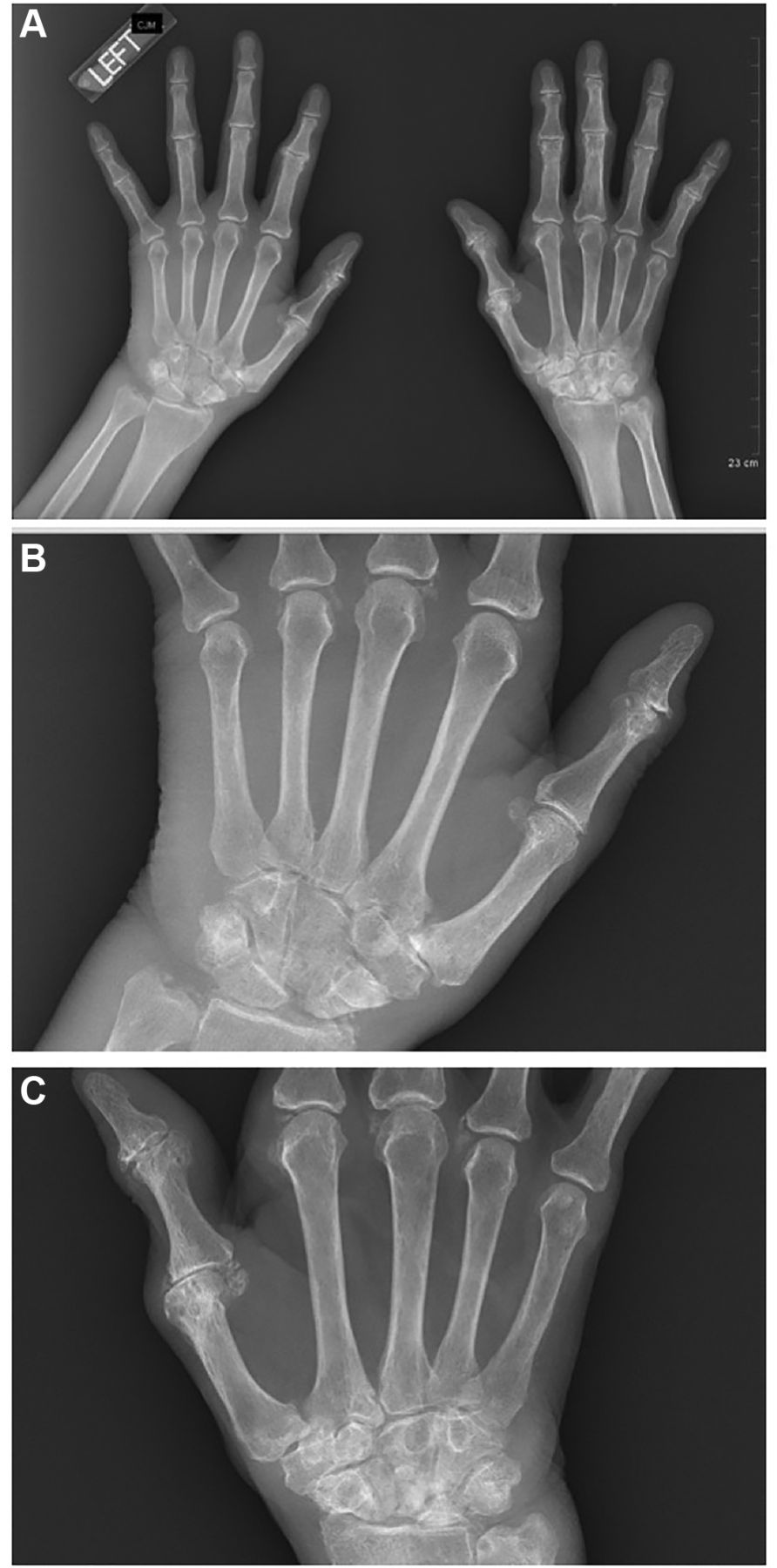
A 77-year-old African-American woman with a new suspected diagnosis of RA initially presented to the rheumatology clinic with a primary complaint of joint pain in the hands, digits, knees and right ankle to initiate medical management. Her history included end-stage renal disease (ESRD), congestive heart failure and a parathyroidectomy for a parathyroid adenoma a year prior to initial presentation to our clinic. Plain radiographs of the hands and wrists showed chondrocalcinosis, scapho-lunate interval widening and lucencies within the right scaphoid, capitate and lunate bones (figures 1A, B and C). Plain radiographs of the knees (figure 2) and right ankle (figure 3) also showed femorotibial chondrocalcinosis. These radiographic findings, combined, support a diagnosis of CPPD. The diagnosis was confirmed by an inflammatory synovial aspirate of the right knee containing CPP crystals and 4203 nucleated cells/μ L. Laboratory tests to rule out secondary causes of CPPD at the time of visit included: corrected calcium 8.7 mg/dL (normal 8.9–10.2), ionised calcium 2.9 mg/dL (normal 4.6–5.1), phosphorous 4.1 mg/dL (normal 2.5–4.5), magnesium 2.0 mg/dL (normal 1.9–2.4), and both liver studies and a complete blood count (CBC) fully within reference range. Initially her joint pain and attacks were refractory to oral prednisone 15 mg daily; non-steroidal anti-inflammatory drugs and colchicine were both contraindicated due to ESRD. She required wheelchair assistance to her appointments.

(A) Hands and wrists: degenerative changes at the thumb CMC articulation. Chondrocalcinosis at thumb, index, middle and ring finger MCP joints. PIP joint space narrowing with demineralisation at the index and middle finger PIP joint. (B) Left hand and left wrist: scapholunate widening. Irregularity of ulnar styloid with chondrocalcinosis involving triangular fibrocartilage complex. Rounded lucencies in capitate, scaphoid and lunate. Degenerative changes at the thumb CMC articulation. Chondrocalcinosis at thumb, index, middle and ring finger MCP joints. PIP joint space narrowing with demineralisation at the index and middle finger PIP joint. (C) Right hand and right wrist: radiocarpal joint space narrowing. Rounded lucency radial aspect of ulnar styloid. Extensive sclerosis of lunate. Lucencies seen throughout carpal bones including scaphoid, triquetrum, lunate and capitate. Chondrocalcinosis at thumb, index, middle and ring finger metacarpal phalangeal joints. Triangular fibrocartilage chondrocalcinosis. CMC, carpometacarpal; MCP, metacarpophalangeal; PIP, proximal interphalangeal.

Right knee: femorotibial chondrocalcinosis.
{kind=link}
{kind=link}
{kind=link}
Right ankle: chondrocalcinosis at first tarsometatarsal articulation.
Two months later, she developed acute synovitis in the right ankle (synovial fluid containing CPPD crystals and 39 090 nucleated cells/μL, but cultures were negative). She was found to have concomitant Streptococcus pneumonia (positive streptococcus urine antigen and lobar infiltrate, but no bacteraemia) and subsequent cardiomyopathy. Her hospital course lasted 4 weeks, during which time her sepsis resolved with treatment, and she achieved clinical remission of her pseudogout flare with an oral prednisone 30 mg taper regimen.
Outcome and follow-up
She has since been in remission of CPPD attacks while on chronic oral prednisone 4 mg daily. Injectable therapies were offered; however, the patient declined parenteral therapy as she does not want to be subjected to needles. She denies having any subsequent acute attacks but reports mild chronic knee and hand pain. She no longer requires wheelchair assistance.
Discussion
Differentiation of CPPD from other arthritides with radiographs is a key diagnostic step and helps determine disease burden. Although CPPD is known to typically cause chondrocalcinosis in the knees and wrists, in more severe cases the second and third MCP joints are also affected.12 Most notably in our patient, chondrocalcinosis is additionally present bilaterally in the fourth and fifth MCP joints as well as the right thumb MCP joint. The deposition of CPP crystals in the fourth and fifth MCP joints is highly unusual, and is perhaps due to our patient’s concomitant OA, ESRD and prior hyperparathyroidism from a parathyroid adenoma. OA of the knee, wrist or MCP joints carries an increased risk of future CPP deposition in the same joint, and also increases the risk of CPP deposition in general.5 This patient’s chronic CPPD is less likely due to other secondary causes given the metabolic values mentioned above. Haemochromatosis is also an important predisposing factor to rule out.3 However, the gastroenterologist recommended not checking iron studies given her normal liver studies. Acute CPP deposition is also known to be a sequela of acute severe infection, which our patient developed.1 Her presentation highlights the importance of early identification and treatment of potential secondary causes of an acute pseudogout attack.
Even at low doses, corticosteroid therapy has moderate success in CPPD for prophylaxis and can diminish the inflammatory response.13 Prednisone can further increase the propensity to develop osteoporosis in patients with CPPD and comorbid risk factors already associated with osteopaenia, specifically: hyperparathyroidism, ESRD and thyroxine replacement. Prednisone doses >7.5 mg have been suggested to contribute to increased risk of infection in a population with ESRD in which infection is the leading cause of death, via dialysis access devices and non-access.14
With further understanding of the inflammatory cascade involved in CPPD and knowledge of interleukin-1β as the main cytokine responsible for the pseudogout inflammatory response, interleukin-1β inhibitors (anakinra, canakinumab and rilonacept) are being investigated as therapy. There have been case reports and case series of success with interleukin-1β inhibitors for both prophylaxis and treatment in patients with ESRD.15 16 However, there are no randomised controlled clinical studies to support efficacy. Furthermore, these therapies are only administered parenterally (which excludes our patient from treatment given her aversion to needles), and the cost of therapy can exceed US$100 000 annually.
This case report highlights a 77-year-old woman with chronic CPPD on low-dose prednisone therapy due to contraindications for first-line therapy, who has a significant burden of chondrocalcinosis in her knees, wrists and MCP joints leading to a false-diagnosis of RA initially. Treating chronic arthritides in the setting of multiple comorbidities is both common and challenging. Alternative medical and non-medical strategies are not well established. Further research is necessary to investigate the benefits of novel selective therapies in the management of chronic CPPD. In addition, it is important to recognise that any acute CPPD attack may be a harbinger of often a more ‘critical’ systemic process.
Learning points
Calcium pyrophosphate deposition disease (CPPD) is a disease of the joints caused by calcium pyrophosphate deposition.
It is rare to see chondrocalcinosis in all metacarpophalangeal joints.
An acute CPPD attack may be a response to an underlying infection.
Comorbidities such as end-stage renal disease limit options for therapy and make treatment a challenge.
New therapies have yet to be validated, but interleukin-1β inhibitors may be a promising future therapy.
References
Footnotes
Contributors CAR, TCS and KML contributed to design, critical review, final approval and integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.