Article Text

Statistics from Altmetric.com
Description
A 27-year-old man presented with a history of 4-year duration of mechanical pain in the left shoulder and a progressive reduction in the range of movements. In the physical examination stands out a swelling of stony consistency on the posterior aspect of the left arm, pain with all active and passive movements of the left shoulder associated with limitation of active and passive abduction above 90°.
The blood tests were normal. The X-ray of the left shoulder showed multiple calcified intra-articular and extra-articular loose bodies (figure 1).

Conventional left shoulder radiography: multiple calcified intra-articular and extra-articular bodies.
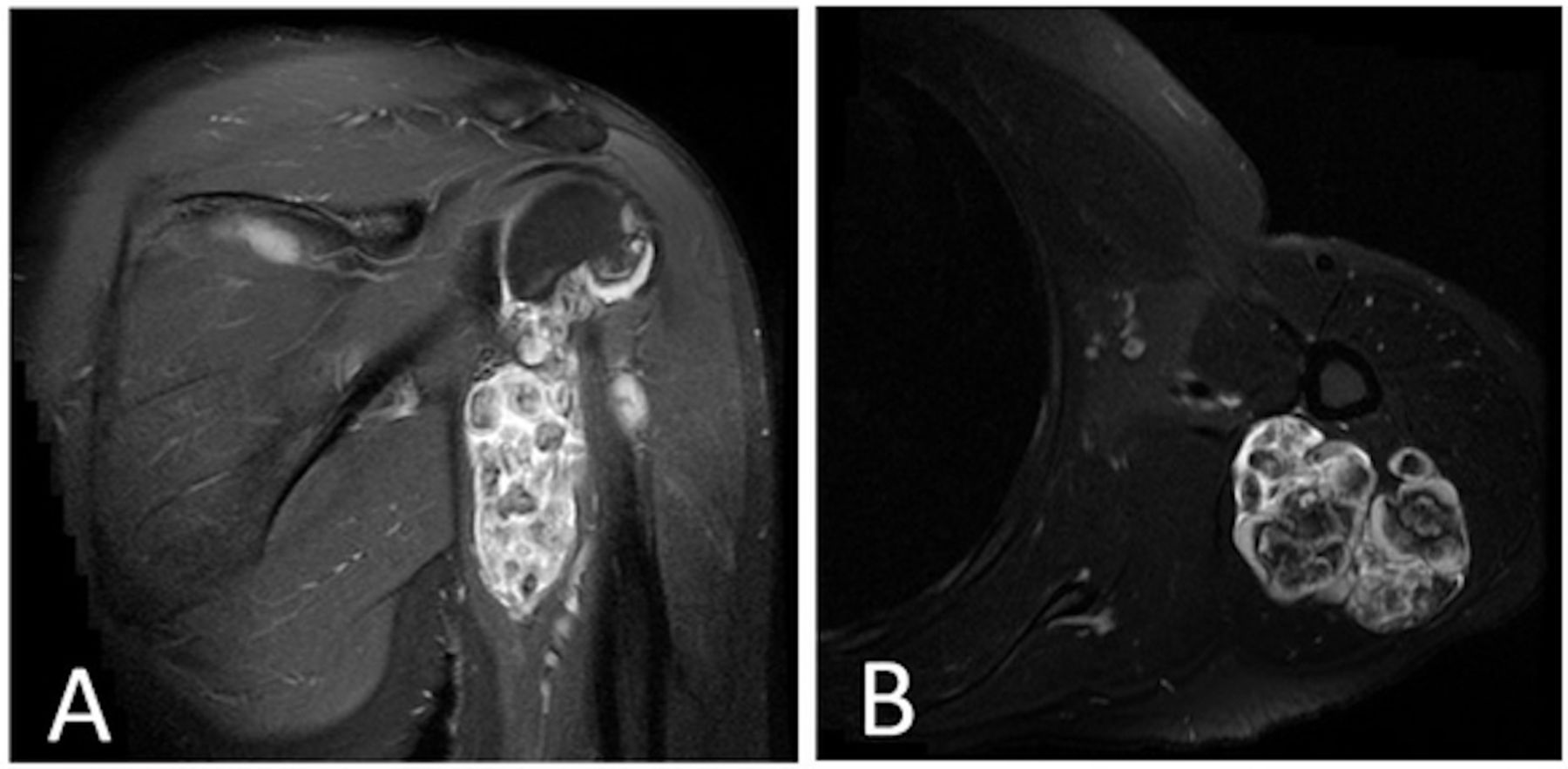
A shoulder MRI was ordered demonstrating exuberant expansion of all joint spaces and recesses from the glenohumeral interface to the subcoracoid and subscapularis recess and along the tendon sheath of the long portion of the biceps, which suggested cartilaginous nature with associated calcification (figure 2A,B). A CT-guided synovial biopsy was performed, and the histology confirmed the diagnosis of synovial chondromatosis. The patient was submitted to arthroscopic examination, and excision of all loose bodies was associated with synovectomy. He was discharged 4 days later, without any clinical intercurrence, and he returned to his physical activities 3 months after discharge.

{kind=link}
{kind=link}
MRI of the left shoulder (T2-weighted sequences with fat suppression): exuberant expansion of all joint spaces and recesses from the glenohumeral interface to the subcoracoid and subscapularis recess and along the long biceps tendon sheath, which suggests cartilaginous nature, with associated calcification.
Synovial chondromatosis (also known as Reichel-Jones-Henderson syndrome) is a rare and usually monoarticular disorder of synovial joints, characterised by the formation of multiple foci of cartilage in the synovial subintima and with multiple intra-articular loose bodies associated.1 Although any synovial joint may be affected, it rarely involves the shoulder joint (about 5% of the cases), and extra-articular extension is even quite rare.2 3 Synovial chondromatosis occurs as either in a primary (without identifiable joint pathology) or secondary form (in the setting of pre-existent osteoarthritis, rheumatoid arthritis or other joint conditions).3 The diagnosis is obtained by histological evidence of cartilage production in the synovial membrane, as the result of synovial metaplasia.3 In current practice, most authors agree that arthroscopic removal of loose bodies for mechanical symptoms is the best surgical treatment.3
The authors highlight this case because of the uncommon diagnosis and location, associated with an exuberant joint distension and extra-articular extension, in the presence of a common musculoskeletal complaint.
Learning points
Synovial chondromatosis is a rare, benign condition.
The most frequent site of involvement is the knee, followed in descending order of frequency by the hip, shoulder, elbow and ankle.
Synovial chondromatosis may lead to articular damage and subsequent development of osteoarthritis.
Arthroscopic management is appropriate for disease isolated to the knee, shoulder and hip.
Footnotes
Contributors FC and JPF wrote the manuscript and performed a review of the literature. MC and AM contributed to critical revision of the article and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.