Article Text

Statistics from Altmetric.com
Description
Ectopic thyroid tissue (ETT) occurs due to a disorder in the embryonic development of the thyroid gland with incomplete migration of the thyroid tissue from the median plate of the floor of the pharyngeal gut to its usual site. ETT is a rare entity, with an estimated prevalence of 1/100 000–300 000 in the general population, increasing to 1/4000–8000 in patients with thyroid dysfunction. The mechanisms responsible for thyroid morphogenesis have not yet been fully elucidated but certain transcription factors such as TITF1/NKX2-1, PAX8, HHEX or FOXE1 play a key role in this process. ETT mainly affects young women and is often asymptomatic.1 In 90% of the cases, ETT is located at the base of the tongue. The occurrence of two ectopic foci simultaneously is particularly rare.2 The authors present the case of a 30-year-old female patient under endocrinology’s care due to autoimmune subclinical hypothyroidism. She was medicated with levothyroxine 25 µg/day and an oral contraceptive. There was no other relevant personal history. Her mother had a benign nodular thyroid disease. On examination there was a midline neck lesion, at the level of the hyoid bone, suggestive of a thyroglossal cyst. The lump had well-defined boundaries and a smooth surface. No other lumps were detected on physical examination. A neck ultrasound (US) was requested and it revealed two structures compatible with ETT at the medial prehyoid region with 14×9 mm and at the base of the tongue with 16×15 mm and absent orthotopic thyroid tissue. She underwent a cervical MRI which confirmed US findings. Subsequently, a radionuclide scan with technetium-99m showed uptake in two foci consistent with sublingual and prehyoid ETT, and no thyroid tissue was observed in the normal thyroid bed (figures 1 and 2). The patient will maintain annual follow-up with neck US and thyroid function tests and periodic MRI. Dual ectopic thyroid gland is a rare clinical entity, for which a high degree of clinical suspicion is required.

Scintigraphy with pertechnetate: the dynamic study shows radionuclide uptake at the base of the tongue and at the prehyoid region, whereas orthotopic thyroid is absent.

{kind=link}
{kind=link}
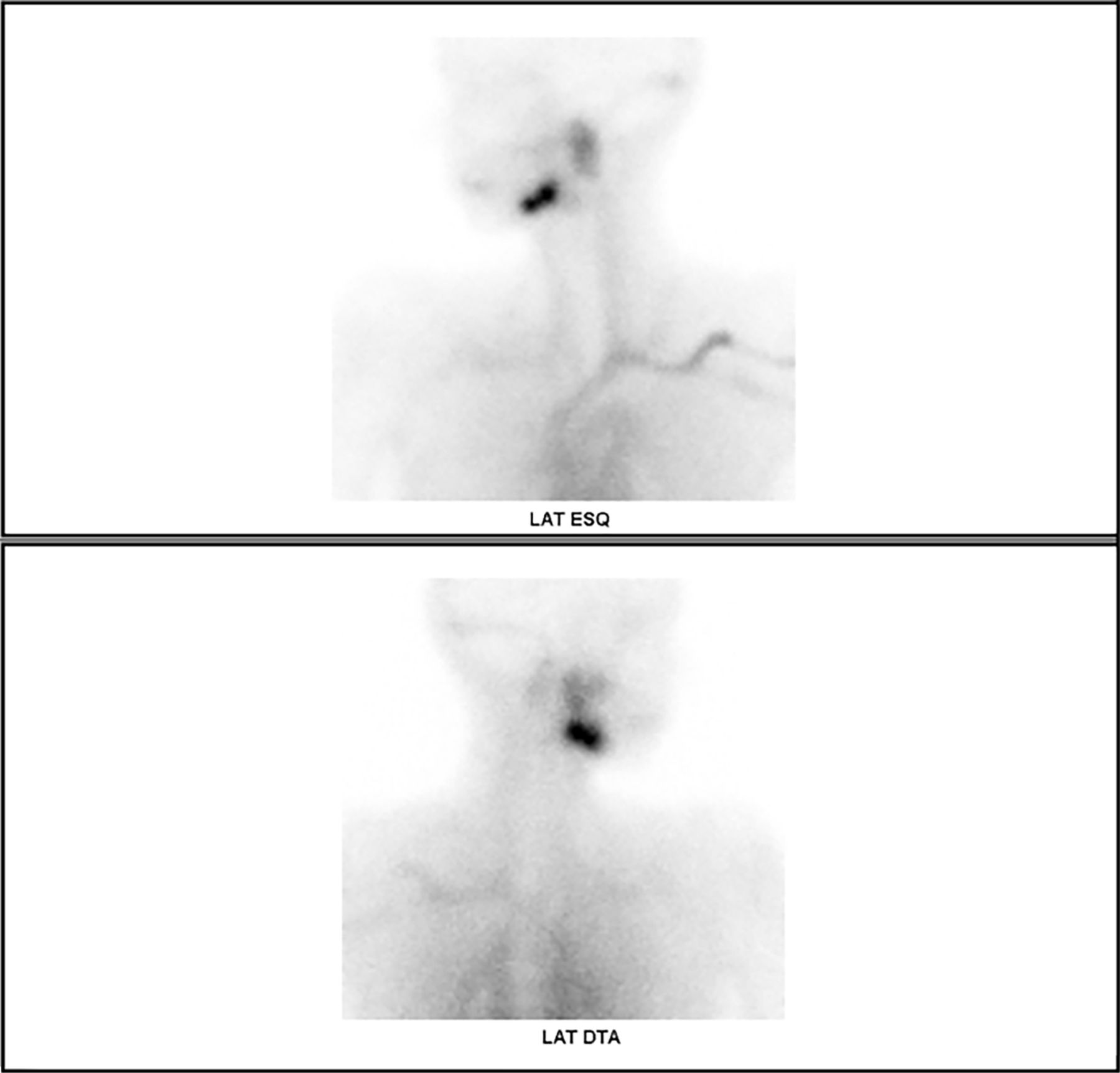
Scintigraphy with pertechnetate: the right and left static lateral views show radionuclide uptake at the base of the tongue and at the prehyoid region, whereas orthotopic thyroid is absent.
The gold standard for ETT diagnosis is thyroid scintigraphy. Furthermore, thyroid scintigraphy allows to differentiate EET from other causes of midline cervical masses such as thyroglossal duct cyst, lipoma, enlarged lymph node, epidermoid cyst, vascular malformation and malignancies. Therefore, recognising ETT may avoid inappropriate surgery.3
The treatment approach is not consensual and it depends on the clinical presentation. While small lesions require no therapy, in case of airway obstruction or repeated haemorrhage, surgical excision may be indicated.
Learning points
Dual ectopic thyroid gland is a rare clinical entity.
Scintigraphy with technetium-99m is the gold standard for ectopic thyroid tissue diagnosis, confirming the location and extension of the ectopic thyroid tissue and the presence or absence of the thyroid gland in its normal anatomic position.
Treatment depends on the clinical presentation and surgical treatment may be indicated in symptomatic cases.
Acknowledgments
We thank Professor Valeriano Leite and Dr Teresa Ferreira.
Footnotes
Contributors CMC wrote the manuscript. SD and MC cooperated in the writing of the manuscript and subtitle of the figure. HV reviewed and corrected the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.