Article Text

Statistics from Altmetric.com
Description
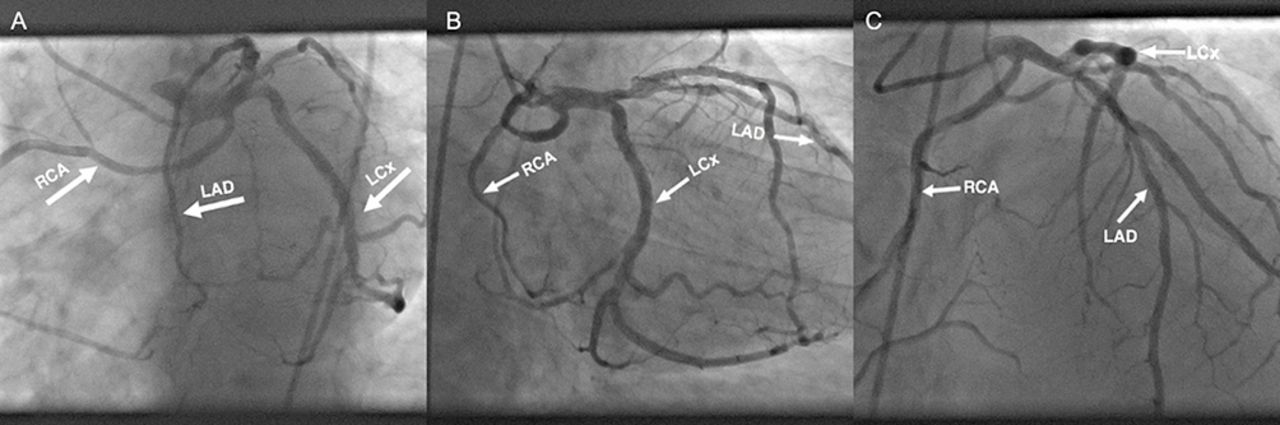
A 45-year-old man with known history of coronary artery disease and bicuspid aortic valve (BAV) (figure 1) was admitted for worsening symptoms of angina. Coronary angiogram showed single coronary artery arising from the left cusp, trifurcating into right coronary artery, left anterior descending (LAD) and left circumflex artery (LCx) (figure 2). No course of the left main coronary artery between the aortic root and the pulmonary artery was noted. There was obstructive disease in proximal LAD (70%), first diagonal artery (80%) and proximal LCx (70%). Peak gradient of 51 mm Hg across the BAV was registered. He underwent bypass graft surgery along with an aortic valve replacement successfully.

Transoesophageal echocardiogram. Parasternal short axis view revealing bicuspid aortic valve (BAV). Red arrows pointing at aortic valve cusps.
{kind=link}
{kind=link}
(A) Left anterior oblique (LAO) caudal view. (B) Right anterior oblique (RAO) caudal view. (C) Anterior-posterior (AP) cranial view. LAD, left anterior descending artery; LCx, left circumflex artery; RCA, right coronary artery.
Single coronary artery is an extremely rare condition with a prevalence ranging from 0.0024% to 0.044%. This variance may be associated with another congenital heart diseases, decreased myocardial perfusion and increased risk of sudden cardiac death.1 Identification of anomalous coronary arteries (ACA) before planned surgery is crucial as it may carry significant technical difficulties. It is also important to recognise the malignant course of ACA as it warrants further evaluation.2
Learning points
Association between anomalous coronary arteries and other congenital heart disease.
The importance of recognition of the anomalous coronary arteries anatomy.
Footnotes
Contributors DMZ, YA, GST and JK were the physicians in charge of the patient throughout hospitalisation and follow-up. DMZ and JK were responsible for performing, diagnosing and discussing the imaging studies of the patient. DMZ prepared the manuscript draft, which was critically revised by YA, GST and JK and approved by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.