Article Text

Statistics from Altmetric.com
Description
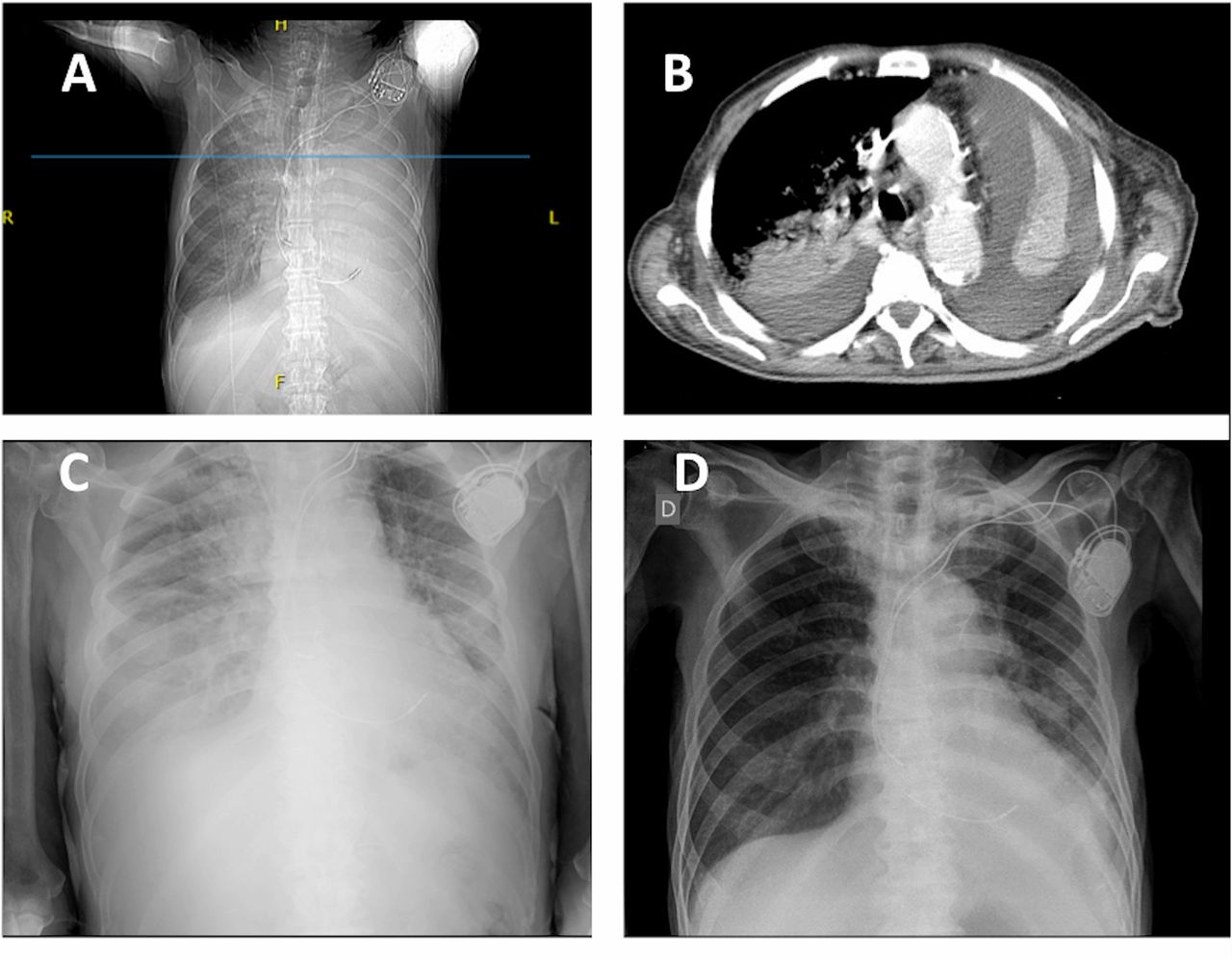
An 82-year-old man presented with hypoxaemic respiratory insufficiency due to left-sided pneumonia and lung atelectasis, with a large, long-standing (>7 days) ipsilateral pleural effusion (figure 1A,B). Four hours after draining 1500 mL of transudative pleural fluid, the patient had worsening hypoxaemia and increasing supplemental oxygen necessity (fractional inspired oxygen 60% with high-flow face mask). The left lung had expanded, as noted by normal vesicular lung sounds, while diffuse crackles were exhibited on the right side. The chest radiograph (figure 1C) shows asymmetrical diffuse alveolar opacity in the right lung field, which in this setting relates to non-cardiogenic pulmonary oedema after contralateral pulmonary re-expansion. After 12 days of conservative treatment, the patient was well, his left lung was expanded and his right-sided oedema had completely resolved (figure 1D), with no need for supplemental oxygen.
{kind=link}
(A) Chest X-ray showing a left-sided pneumonia and atelectasis with a large pleural effusion of at least 7 days in a patient with partial respiratory insufficiency. (B) CT showing the collapsed left lung and large ipsilateral pleural effusion at the level of the aortic arch (blue line on image A). (C) Asymmetrical, right-sided, non-cardiogenic acute pulmonary oedema with aggravated hypoxaemia after left-sided pleural effusion drainage and pulmonary re-expansion. (D) Chest X-ray after resolved pulmonary oedema and pleural effusion with clinical stability and no need for oxygen supplementation.
This case reports an acute non-cardiogenic pulmonary oedema due to contralateral pulmonary re-expansion after pleural effusion drainage, adding to the scarce literature of this rare yet clinically meaningful event. It is unique as oedema is noted asymmetrically and mostly evident contralateral to thoracentesis.
The pathogenesis of this phenomenon is unknown and only five previous cases have had similar findings. In a previous report, overperfusion of the contralateral lung was thought to be the main mechanism for re-expansion pulmonary oedema (RPO). The patient had a hepatopulmonary syndrome and uneven pulmonary vasoconstriction of the ipsilateral lung, as a result of hypoxaemia related to an intrapulmonary shunt.1 In our case, whether overperfusion and/or contralateral lung underlying disease (eg, right lower lobe atelectasis, as noted by deviated trachea) must be present for contralateral RPO could be argued. On a cellular level, polymorphonuclear leucocytes have been implicated, yet inflammation was less severe contralaterally.2 Other investigations show a fundamental role of both leucocytes and platelets for contralateral RPO.3
Similarly, the pathophysiology of ipsilateral oedema is not completely defined. An increase in microvascular permeability and ensuing lesion secondary to free radicals is often proposed as the main mechanism to ipsilateral re-expansion of the lung leading to ischaemic-reperfusion injury. Accordingly, one would expect the ipsilateral lung to be the most affected. In contrast, we here presented a rare case with the contralateral lung being the most distressed.
In conclusion, RPO, an infrequent but life-threatening condition, occurs mostly in the affected collapsed lung. Given the potential mechanisms, the British Thoracic Society 2010 Guidelines recommend avoiding high intrapleural pressures during the procedures, draining no more than 1.5 L in the first hour. Younger patients, those with large pleural effusions or pneumothoraces and collapsed lung for >7 days, are at greater risk. Adequate supplemental oxygen and ventilation are paramount to successful treatment. Whether diuretics, bronchodilators or steroids are of added benefit is unproven. Moreover, whether these findings also apply to contralateral RPO is unknown, and future investigation is hampered by the scarcity of this event.
Learning points
Acute non-cardiogenic pulmonary oedema after contralateral pleural effusion drainage is a rare but life-threatening thoracentesis complication.
Early recognition of this clinical entity and adequate supportive treatment constitute the mainstay of treatment.
Acknowledgments
Professor Candida Fonseca (collaborator) did a critical revision of the final version for submission. Gonçalo Cunha (contributor) did image formatting and design.
Footnotes
RG and BR contributed equally.
Contributors RG and BR: design of the case report, acquisition, analysis and interpretation of the data, and first draft and final reviewed version of this work. BR and RG (joint first authorship): contributed equally to the final version of this manuscript. RM and IA: interpretation of the data, critical revision of the first draft and approval of the final version of this manuscript. All the authors, collaborator and contributor have approved the final version of the manuscript. The collaborator and contributor have given us written permission to be acknowledged in this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.