Article Text

Statistics from Altmetric.com
Description
A 25-year-old female patient was referred to our eye emergency when she noticed sudden painless diminution of vision in both eyes within 6 hours of an uncomplicated vaginal delivery of a full-term healthy neonate with a birth weight of 2.8 kg. There was no history of prior pregnancies and antenatal or perinatal illness during the present pregnancy, that is, no association of anaemia, coagulopathy, pre-eclampsia or hyperemesis. There was no requirement of episiotomy, forceps or vacuum during delivery. No labour-inducing or epidural anaesthetic agents were used. Fundus examination was normal in the antenatal ophthalmic records on fourth-month and eighth-month follow-up visits.
The patient’s blood pressure was 124/74 mm Hg and pulse rate was 82 beats per minute. Vision was counting fingers close to face in both eyes. On slit lamp examination, anterior segment was normal in both eyes with retrolental red blood cells visible. On fundus examination, we found that there was bilateral vitreous haemorrhage with subhyaloid haemorrhage in the right eye. Optomap (Optos, Tokyo, Japan) ultrawide field fundus retinography was performed for documentation [figure 1A, B]. Ocular ultrasonography revealed vitreous and subhyaloid haemorrhage in both eyes corroborating with our clinical findings (figure 2A, B). Thus a diagnosis of bilateral valsalva retinopathy was made as the aforementioned clinical picture occurred soon after labour. In view of bilaterality, an early pars plana vitrectomy was performed in the left eye while right eye was operated after 3 months as the haemorrhages did not resolve spontaneously till then. Snellen visual acuity improved to 20/40 in the left eye and 20/50 in the right eye on subsequent follow-up visit.

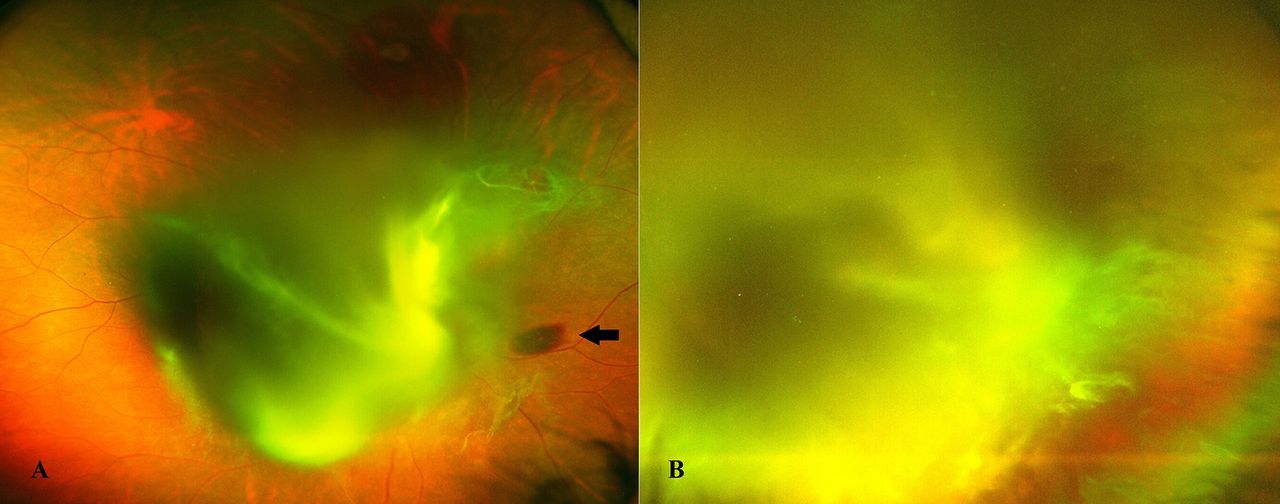
Optomap ultrawide field fundus retinography showing bilateral vitreous haemorrhage (A, B) along with subhyaloid haemorrhage in the right eye (black arrow) (A).
{kind=link}
{kind=link}
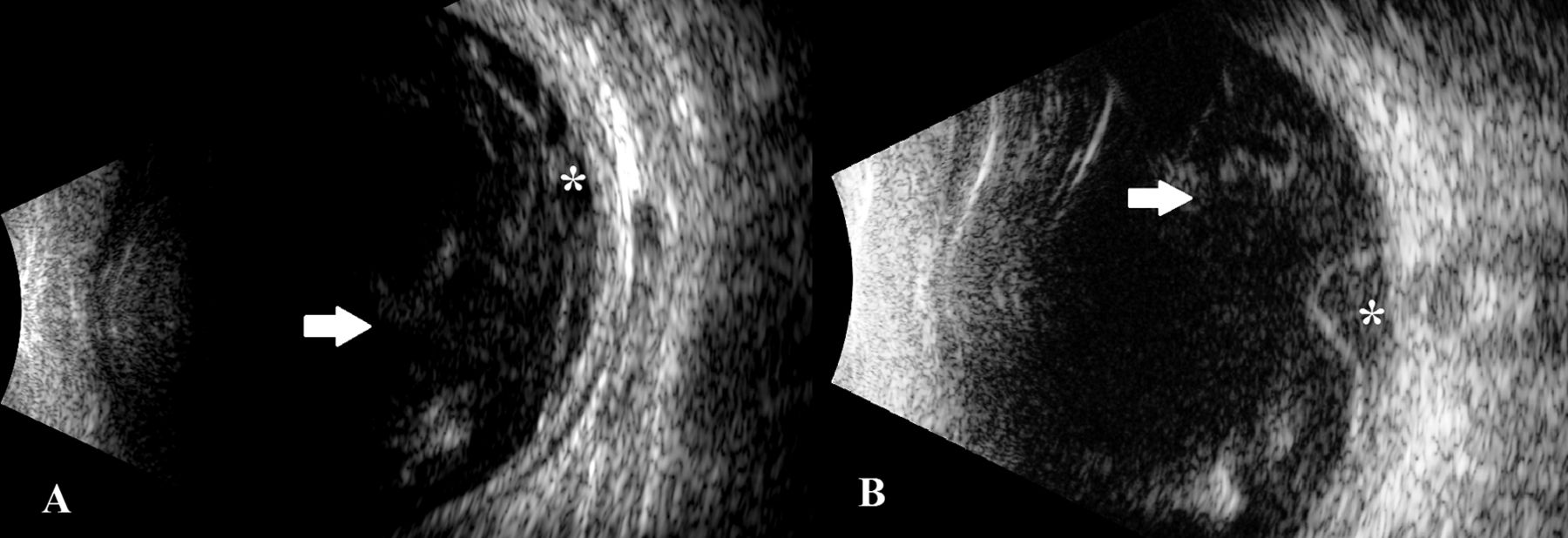
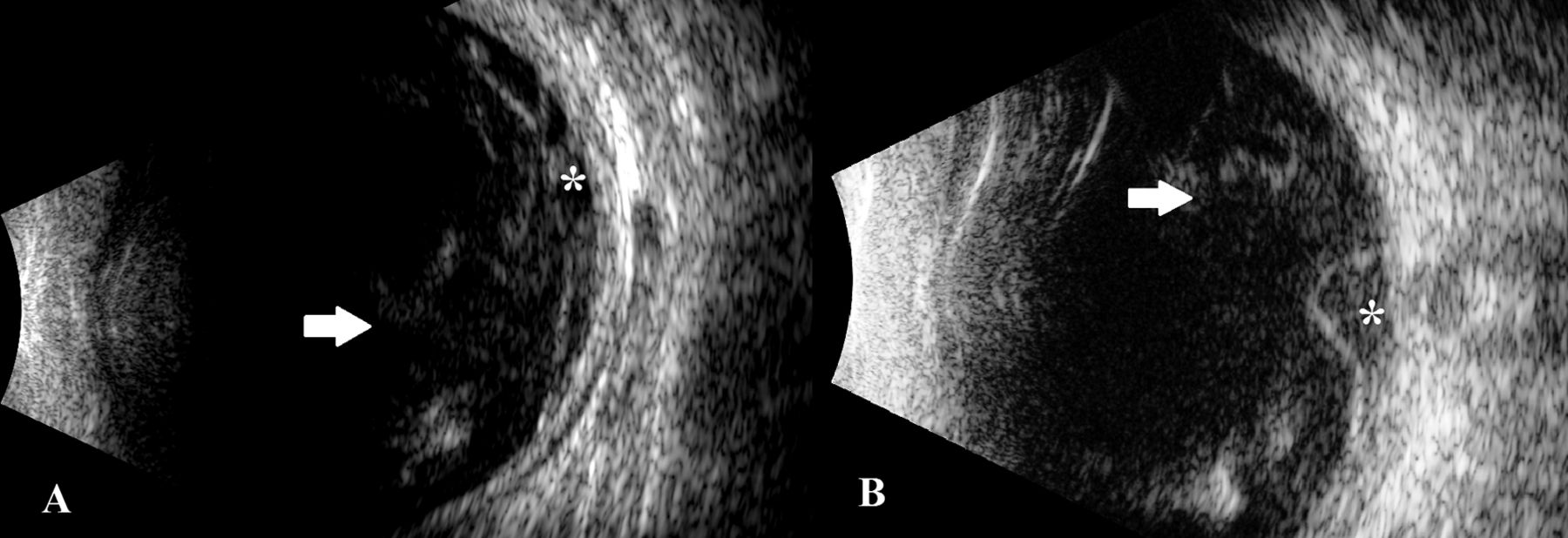
Ocular ultrasonography of the right eye (A) and the left eye (B) showing vitreous haemorrhage (white arrows) and subhyaloid haemorrhage (white asterisks).
Valsalva retinopathy comprises preretinal haemorrhages soon after forceful exhalation with closed glottis due to sudden increase in intrathoracic and intra-abdominal pressure. Vast array of conditions have been linked with valsalva retinopathy such as constipation, pregnancy, sneezing, coughing, weightlifting and coitus. Most commonly valsalva retinopathy is unilateral.1 Since its first description, there is minimal published data on bilateral valsalva retinopathy and all the cases described have associated comorbidities like proliferative diabetic retinopathy, anaemia, leukaemia and trauma.2 3 These can be cumulatively termed as ‘valsalva-like retinopathies’. To the best of our knowledge, bilateral ‘true’ valsalva retinopathy has not been described in the literature.
Valsalva retinopathy during and after pregnancy may be precipitated by hyperemesis, anaemia and labour. In our case, labour was the culprit although uncomplicated. We hypothesise that lack of maintenance of lateral decubitus position during the third trimester of pregnancy may cause prolonged decompression of abdominal veins which may lead to rise in the peripheral venous pressure and thereby causing rupture of intraocular venules and capillaries during labour, risk of which is accentuated by infrequent breathing. Labour should be aided with episiotomy, forceps or vacuum when feasible and frequent breathing should be encouraged during the procedure to avoid such grave complications like valsalva retinopathy. Prognosis of valsalva retinopathy is excellent and treatment approaches include observation, neodymium-doped yttrium aluminium garnet hyaloidotomy and vitrectomy for increasing grades of haemorrhages, respectively.3
Learning points
Valsalva retinopathy is more commonly unilateral and bilaterality is of seldom occurrence.
Valsalva retinopathy may occur after an uncomplicated pregnancy with normal vaginal delivery.
Lateral decubitus position during the third trimester and frequent breathing during labour may reduce the risk of valsalva retinopathy.
Footnotes
Contributors VM: hypotheses and manuscript preparation. HKN: image retrieval. PC: case selection and examination. AK: guidance and final editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.