Article Text

Summary
A 29-year-old nulliparous woman with a dichorionic diamniotic (DCDA) twin pregnancy was referred to our hospital at 16 weeks’ gestation for prenatal diagnosis. She was diagnosed of Haemoglobin H Constant Spring (Hb H CS; --SEA/αCSα) and her husband of alpha thalassemia-1 trait (--SEA/αα). Detailed ultrasound showed that left twin had fetal anaemia and early signs of hydrops while the right one was normal. Both twins were female. Amniocentesis in each sac was performed for prenatal diagnosis of thalassemia after a proper counselling with the couple. DNA analysis confirmed that the left fetus was affected with haemoglobin Bart’s hydrops fetalis (--SEA/--SEA) while the right one was alpha thalassemia-1 trait (--SEA/αα). Selective feticide with intracardiac injection of KCl was successfully performed on the hydropic fetus. Identification of the affected fetus is crucial for selective termination. Family counselling about the procedure and complications is also necessary.
- genetic screening / counselling
- pregnancy
- materno-fetal medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Haemoglobin (Hb) Bart’s hydrops fetalis is the most severe form of thalassaemia, arising when a fetus inherits alpha thalassaemia-1 genes from both parents. The severity of the condition is such that the affected fetus succumbs in utero or soon after birth. In this condition, almost all the produced haemoglobin (Hb Bart’s) would not deliver oxygen to all body tissues, resulting in severe tissue hypoxia, causing fetal or neonatal death.1–3 Besides, a pregnant woman carrying a fetus with Hb Bart’s hydrops fetalis is at risk of pre-eclampsia and postpartum haemorrhage, both of which can cause severe maternal morbidity or even mortality.4
Currently, various prevention and control programmes for severe thalassaemia have been established worldwide including in Thailand and prenatal diagnosis for severe thalassaemia diseases is available. If a fetus is diagnosed with Hb Bart’s hydrops fetalis, termination of pregnancy is offered due to the reason mentioned earlier.5
The pregnant woman in our case presentation was diagnosed with Hb H constant spring (Hb H CS), thus carrying alpha thalassaemia-1 gene which was identified as –SEA. Her husband was diagnosed with alpha thalassaemia-1 trait which also was identified as –SEA. Therefore, their offspring had a 25% chance of being affected with Hb Bart’s hydrops fetalis and was referred to our hospital for prenatal diagnosis. However, an additional issue was that the woman was pregnant with dichorionic diamniotic (DCDA) twins. Theoretically, twin pregnancies have a higher risk of not only having a baby with genetic diseases, but also procedure-related pregnancy loss.6 7 Furthermore, the identification of fetuses for prenatal diagnosis and treatment as well as options according to the prenatal diagnosis results is more complicated than in singleton pregnancies.
At Faculty of Medicine Siriraj Hospital, prenatal diagnosis for thalassaemia has been set up for >30 years with an increasing number of couples at risk opting for prenatal diagnosis. Currently, the procedure has been performed on approximately 300 cases including 5–10 twin pregnancies annually. In this case report, we present an interesting experience of prenatal diagnosis and management in DCDA twins at risk for Hb Bart’s hydrops fetalis.
Case presentation
A 29-year-old Thai nulliparous pregnant woman with a twin pregnancy was referred to our unit at 16 weeks’ gestation for prenatal diagnosis of thalassaemia. The woman had been diagnosed with non-transfusion-dependent Hb H CS disease with the genotype of --SEA/αCSα. She had needed only 4–5 blood transfusions since birth. Her husband was diagnosed with alpha thalassaemia-1 trait with a molecular diagnosis of --SEA/αα. Her offspring, therefore, had a 25% risk of hydrops fetalis.
Detailed ultrasonographic examination showed two intrauterine gestation sacs. Both twins were female. There were two separated placentae located at anterior and posterior walls of the uterus. The intertwin membrane thickness of >2 mm along with the lambda sign or twin-peak sign was noted (figure 1). These findings were suggestive of DCDA twin pregnancy. The twin at the maternal left side (left-sided fetus) had early signs of hydrops fetalis (figures 2 and 3) with cardiomegaly, increased cardiothoracic ratio (CTR), pericardial effusion and a peak systolic velocity of the middle cerebral artery (MCA-PSV) of >1.5 MoM (38 cm/s). The findings were compatible with fetal anaemia. Placenta of the left-sided fetus was also increased in thickness (placentomegaly). The findings of the right-sided fetus including the placenta were within normal limits.
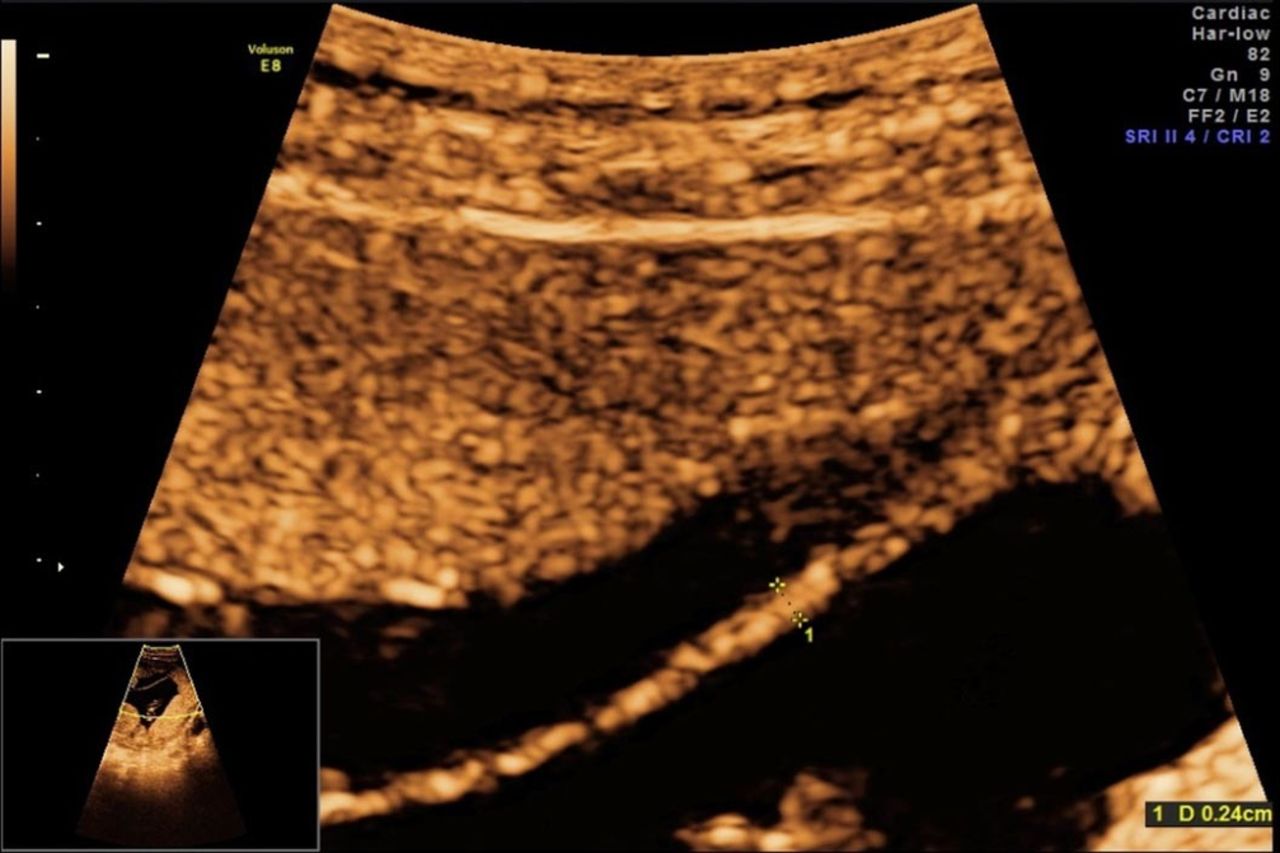
Lambda sign with intertwin membranes >2 mm.

Cardiomegaly with pericardial effusion.

{kind=link}
{kind=link}
{kind=link}
Ascites.
The patient and family were counselled about the risk of the invasive procedure against the approximately 50% risk of having at least one fetus being affected with severe thalassaemia and also the increased probability of the left-sided fetus being hydrops fetalis from the ultrasound findings. Various possible results and management options were discussed. The couple decided to have the invasive procedure performed. At 17 weeks of gestation, amniocentesis was done for each sac and the samples were sent for DNA analysis. The results confirmed 2 weeks later that the left-sided fetus was indeed affected while the right-sided twin was diagnosed as an alpha thalassaemia-1 carrier (--SEA/αα).
Selective feticide was offered to decrease the risk of complication such as pre-eclampsia or postpartum haemorrhage which could result in morbidity or mortality of the woman and the remaining fetus. The patient and her husband accepted the procedure-related complications including amniotic leakage, vaginal bleeding, co-twin death and abortion. Intracardiac injection under the ultrasonographic guidance of potassium chloride (KCl) with a concentration of 2 mEq/10 mL was slowly performed on the fetus with hydropic features until fetal asystole was observed for 3 min then the needle was removed. The total amount of KCl used was 15 mL. A repeated scan was done at 30 min later to confirm the fetal death. After the successful procedure, the patient was admitted to monitoring for any complications for 1 day. Unexpectedly, the left-sided fetus resumed heart activity with a normal fetal heart rate (FHR) observed by ultrasonographic scan on the next day. The procedure of KCl injection was repeated after counselling. Intracardiac injection of KCl was increased to 40 mL with a concentration of 2 mEq/10 mL by the same technique and FHR was perpetually absent finally.
Outcome and follow-up
The patient was scheduled for antenatal visits at the high-risk pregnancy clinic every 2–3 weeks. During the pregnancy, the patient needed packed red cell transfusions every 4–5 weeks to keep Hb levels to >8 g/dL. Serial ultrasonographic scans were performed for growth evaluation of the remaining fetus.
The patient came to the hospital with regular uterine contractions every 5 min at 30 weeks’ gestation. Pelvic examination showed the cervical dilatation of 3 cm with 50% effacement. The cause of preterm labour could not be identified. A course of steroid was given to enhance fetal lung maturity along with the inhibition of labour during the course of steroid administration. On the eighth day of admission, the labour progressed into the active phase during which MgSO4 was intravenously administered for fetal neuroprophylaxis. The patient delivered vaginally a 1620 g female baby with Apgar scores of 7.9 along with a small macerated dead fetus. The woman could be discharged on day 2 postpartum while the baby was treated for prematurity and could be discharged on day 39. Subsequent development of the baby had been normal as of the time of this report (aged 1 year and 2 months).
Discussion
Twin pregnancies have a higher risk of having a child with a genetic disease than singleton pregnancies, especially in a dizygotic twin gestation.6 7 Zygosity can be surmised in most cases by determination of chorionicity and amnionicity by ultrasonography in the first trimester or before 16 weeks of gestation.8 9 Monochorionic twins are almost always monozygotic while the majority (90%) of dichorionic twins are dizygotic.8 10 Thus, the genetic makeup of dichorionic twins can differ and invasive prenatal diagnosis must be performed from each sac separately, resulting in increased procedure-related pregnancy loss rate compared with that in singleton pregnancies. Several studies have reported the procedure-related pregnancy loss in twins to be 2%–5%.6 7
Compared with singleton pregnancies, the risk of at least one fetus being affected with severe thalassaemia in a dizygotic twin pregnancy is about double and this information should be given to the couple at risk along with the risk of invasive procedure during the counselling. Furthermore, the couple should be made aware of possible situations of prenatal diagnosis result so that they can make a proper decision about the whole process or consider in advance regarding options after the result becomes available. In other words, they should be informed about options for the following situations: (1) neither fetus is affected, (2) both fetuses are affected and (3) only one fetus is affected. The last situation can cause a dilemma in decision-making.11 12 If pregnancy is continued, they have to prepare for an affected child and the condition puts the woman at risk of mirror syndrome or pre-eclampsia and postpartum haemorrhage.4 If pregnancy is disrupted, the unaffected fetus would be terminated as well.
Another possible option that can be offered for cases with only one affected fetus in a twin pregnancy is selective termination. Risks of the procedure should be discussed such as procedure-related pregnancy loss. Meticulous mapping of each fetal location (and gender, if different) during invasive prenatal diagnosis procedure is crucial so that if selective termination is the chosen option, the operation would be correctly performed on the affected fetus.13 14 Favourably, an affected fetus with hydrops fetalis often exhibits certain ultrasonographic findings which help in identification for selective termination. These findings (cardiomegaly, placentomegaly and increasing of MVA-PSV) could imply fetal anaemia. Some of these signs have been shown to be detectable as early as 11–12 weeks of gestation.15 16 In more advanced cases, ultrasonographic findings of hydrops fetalis such as generalised skin oedema, pleural effusion and ascites can be found.17 18
To perform selective feticide in DCDA twins, many methods are taken into consideration. Ultrasonic-guided injection of 2 mEq/mL KCl into the fetal heart in early gestation and into the umbilical vein after the gestational age of 26 weeks is a well-established procedure which is technically successful in almost 100% of reported cases.13 19 20 In a DCDA twin pregnancy with separated placantae, the passage of substances from one twin into the circulation of the co-twin is negligible due to the lack of placental anastomoses. For this reason, drugs used to induce fetal asystole can be injected with only a very minimal risk to the other twin.
A previous study showed that the amount of KCl used in feticide increased with advanced gestational age. The amount of 2 mL of 2 mEq/mL KCl is used for a gestational age before 16 weeks and 3–5 mL later in pregnancy.21 22 In this case, we used the dilution of 2mEq/10 mL to minimise serious complication should leakage into the maternal circulation occurred. Previous articles have reported that miscarriage rate increases with the gestational age when the procedure is performed with rates of 5.4% at 9–12 weeks, 8.7% at 13–18 weeks and 9.1% at >25 weeks.13 21 22 During the later period of gestation, the increased risk of miscarriage may result from the greater amount of non-viable tissue after the reduction of one fetus and the greater risk of infection or cytokine release. It is also noted that our case ended up delivering preterm while the case reported by Leung et al had a more favourable outcome.1 This might be because they performed selective termination at the earlier gestation.
Conclusion
DCDA twins have different genetic makeup and, if prenatal diagnosis for any genetic disease is decided on, the procedure needs to be performed on each twin separately. The risk of the disease and of invasive diagnostic procedure, both of which are higher than in singleton pregnancies, should be discussed with the family. Furthermore, intensive counselling is needed to plan in advance for various possible results. Meticulous mapping of the fetal location during invasive prenatal diagnosis procedure is crucial for later identification of the fetuses should selective feticide is needed. In those at risk for Hb Bart’s hydrops fetalis, another hint of an affected fetus could be observed on ultrasonography as signs of fetal anaemia or hydrops become visible. These ultrasonographic findings add more clues to identify which fetus is affected and is to be operated on. Again, complications of selective feticide should be addressed to the couple.
Patient’s perspective
I appreciated about the management from all doctors and staffs. Although I lost my one baby, another is still good. Only one baby makes me and my family happy. Thank you for all staffs. I am glad that my case will be the example for all fellows.
Learning points
Most dichorionic diamniotic (DCDA) twins have different genetic makeup among both fetuses.
Prenatal diagnosis has to be performed on each fetus separately with careful fetal mapping for later fetal identification.
Counselling about prenatal diagnosis in DCDA twins has to emphasised on the increased risk of the disease, the invasive procedure and the options for various scenarios including discordant fetal results.
Selective feticide can be performed by KCl on the fetus correctly identified as affected with Hb Bart’s hydrops fetalis using fetal mapping along with the signs of fetal hydrops on ultrasonography.
Counselling about selective feticide should include the step of the procedure and complications.
References
Footnotes
Contributors TP and PR: developed the idea and planned for case-report working. PR and PS encouraged TP and PL to performed the procedure and supervised for the management. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.