Article Text

Summary
Sodium hypochlorite is a corrosive, highly alkaline (pka=7.52) household product. Ingestion of sodium hypochlorite liquid is common, showing toxicity on the oesophagus and stomach. Nevertheless, cases of sodium hypochlorite ingestions in pellet are rare and the management of them is unknown. We report the case of a 65-year-old man who accidentally swallowed a bleach tablet of 3.5 g. Six hours later, the patient developed an aphonia associated with dysponea stage IV, motivating a nasofibroscopy showing glottis and supraglottic necrosis and oedema for which the patient received intravenous steroids, was intubated and then underwent a tracheotomy. After 2 weeks under tracheotomy, local evolution was favourable allowing a removal of the cannula and a return back home.
- poisoning
- resuscitation
- ear, nose and throat/otolaryngology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Caustic agent ingestion, accidental or voluntary, is a common problem with more than 5000 cases reported each year in the USA.1 Sodium hypochlorite is one of the agents most commonly swallowed in liquid form. Emergency care following this kind of ingestion is documented, as well as its effects on the oesophagus and stomach. However, ingestion of a soluble tablet of sodium hypochlorite is rare. The treatment, as well as possible damage on the pharynx and larynx, remains unknown. Through this report, we are going to describe the ingestion of a tablet of sodium hypochlorite, the clinical presentation, the evolution and our support.
Case presentation
A 65-year-old man, only known, medically, for high blood pressure, accidentally swallowed a tablet of soluble bleach sodium hypochlorite. The patient had an headache and decided to take an acetaminophen tablet that was near the kitchen sink. However, confused by his pain, he took by mistake a tablet of soluble sodium hydroxide (3.5 g of sodium hypochlorite per tablet) followed by a glass of water. He described an immediate burning sensation in his mouth and throat, followed by a severe cough, allowing him to expectorate part of the tablet. He arrived at the emergency room 1 hour after ingestion.
The patient complained only of an odynophagia associated with light dysphonia. He suffered no abdominal pains and drank before coming to the emergency room. Vital signs showed an afebrile and eupnoeic patient, with a blood pressure of 168/82 mm Hg. Physical examination showed no erythema on the lips, in the oral cavity or deep throat. Abdominal examination was normal, without pain during the palpation. Blood tests showed an aligned blood formula, a preserved kidney function and excluded any inflammatory syndrome.
The ear, nose and throat (ENT) specialist made a nasofibroscopy showing a soft laryngeal erythema, without oedema. After sufficient pain treatment with intravenous opioid, the patient described an improvement of the odynophagia and a partial improvement of his voice. Then, the patient was kept under medical supervision in the emergency room for 6 hours postingestion, in anticipation of a new ENT control before a possible return home.
After 6 hours of monitoring, the patient presented a stage IV dyspnoea associated with a severe odynodysphagia and aphonia. A new ENT examination excluded an oral lesion, showing necrotising fibrin of supraglottis and massive bilateral arytenoid oedema significantly decreasing glottis flow by 40%. The visible real vocal folds were described as fine.
Initial management includes 250 mg of solumedrol followed by an awake nasotracheal intubation.
Investigations
After intubation, a pharyngoscopy was realised and confirmed superficial necrosis of dorsal epiglottis extending to vocal folds (figure 1) with transluscent oedema of both arytenoids (figure 2). Flexible gastroscopy showed a superficial 1 cm2 ulcer of proximal oesophagus without any other lesion up to duodenum. The day after, considering the expected slow healing process and to avoid laryngeal synechias, a surgical tracheotomy was performed.
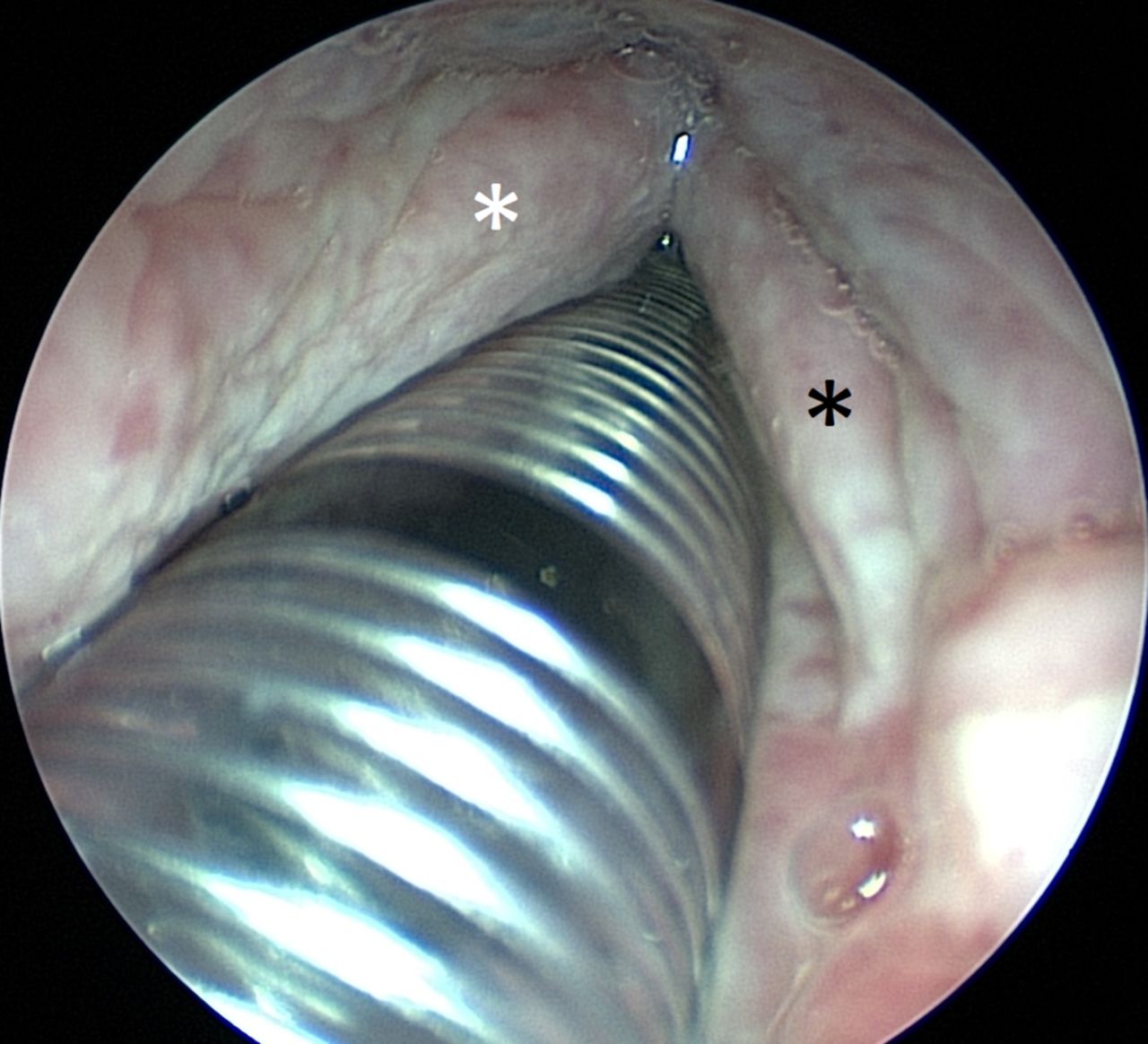
Laryngeal view after intubation. Asterisk represents true vocal folds (black/right side, white/left side, respectively) showing diffuse superficial necrosis.

{kind=link}
{kind=link}
Supraglottic view after intubation. Asterisk represents anterior surface of epiglottis with normal appearance. ↑ : massive oedema of both arytenoids.
Differential diagnosis
The cause of the oedema was the direct irritation of an alkaline product on the laryngeal mucosa. An allergic origin was unlikely.
Treatment
The patient had a tracheotomy for 2 weeks, associated with a proton pump inhibitor treatment (esomeprazol 40 mg) two times per day for 2 days and then one time per day. The patient was hospitalised in intensive care for 2 weeks, where he was given an enteral alimentation via a nasogastric tube only.
Outcome and follow-up
Hospitalisation was complicated by a pulmonary infection, for which an antibiotic treatment was initiated. After 17 days under tracheotomy, the cannula was removed. The patient was given a smooth, then mixed and finally solid diet. ENT follow-up 2 weeks later and then 1 month postingestion confirmed positive local evolution.
Discussion
Ingestion of caustic alkaline product, such as sodium hypochlorite, causes lesions of the mucosa, by a penetrating injury called liquefactive necrosis, allowing deeper tissue damage than acidic substances.2 By aspiration of a tablet of sodium hypochlorite in this patient’s case, the lesions remained mainly high, at the laryngeal level, causing a local necrosis and oedema.
The different guidelines describe support for lesions of the oesophagus and stomach but not for the lesions of the larynx.3 4 The consequences of such ingestion are not known before an endoscopic examination, so it is recommended to offer a similar support the first time. This recommendation is the initiation of a proton pump inhibitor, an endoscopy within 24 hours and a medical supervision.5 6 It should be noted that endoscopy is recommended only for stable patients and without clear evidence of perforation of the oesophagus. It is also best to do X-rays of the thorax and abdomen regularly to exclude an oesophageal perforation. The use of emetic agent, such as coal, or neutralising agent is contraindicated as it can cause vomiting and a new exposure to the irritant product.3 5 7
In the case described above, we decided as a first step to initiate a corticosteroid therapy in view of important laryngeal oedema. Various studies show the absence of benefits from a corticosteroid therapy in the case of oesophageal lesions.8 9 There is no evidence that it is beneficial for laryngeal caustic lesions, but meta-analysis supports its beneficial effect on laryngeal oedema after intubation.10 It has been used in many similar situations, like burns by hot drink or food. Here, a major laryngeal oedema motivated the initiation of this particular treatment, just by a single bolus, with a good clinical evolution.
Also, it was advisable for this patient to perform a nasopharyngeal and awake intubation. This practice is not indicated in the recommendations for the treatment of ingestion of caustic liquids, in view of the risk of vomiting following this intubation and thus re-exposure to the caustic product.3 5 However, in this case, the main problem being the high obstruction of the larynx by the oedema, like in cases of laryngeal oedema in burns, then visualisation was needed for this gesture and early intubation is necessary for upper airway protection.5 11–14 Furthermore, the risk of vomiting and re-exposure to the irritant was low, the patient having ingested it in solid form, with only local irritation and more than 6 hours before.
In this case, the patient presented with a little voice modification but with an improvement after pain killer and a quite normal first nasofibroscopy. This explains why an immediate intubation was estimated overweening. However, an earlier intubation should be discussed in case of severe dysphonia and/or oedema.
Finally, the tracheotomy is the final treatment, the intubation tube being a possible cause of exacerbating irritation and synechias, needed to discharge this area.12 15
On a public health side, this case reminds the importance of appropriate storage for medications and cleaning products.16
Patient’s perspective
I was drowsy, my throat was painful and I could not really talk any more. Much later, an ENT finally came to examine me again: he left quickly and returned with four or five doctors in green clothes. I remember that I needed to urinate but it was denied to me because ‘there was no time’. I don’t have any more memories from this moment and until I got out of coma weeks later. (…) Everyone told me: I came back from a long way. I know I have fought a survival battle, so I wanted to live.
Learning points
Ingestion of sodium hypochlorite in undiluted pellet form is an uncommon but dangerous emergency department complain.
In the absence of specific guidelines, management should be the same as for liquid form.
Steroids and awake nasotracheal fibroscopic intubation should be considered for life-threatening laryngeal oedema.
Footnotes
Contributors CB wrote the first manuscript. FV brought essential contributions and revised the manuscript. CF supervised the whole work and revised the manuscript. All agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published online. The substance ingested by the patient described in the case report was sodium hypochlorite (Bleach, pKa=7.52) and not sodium hydroxide (Caustic soda, pKa=14.8).