Article Text

Summary
Caffeine (1,3,7-trimethylxanthine) is a natural product commonly presented in food’s composition, beverages and medicinal products. Generally, it is thought to be safe under normal dosage, yet it can be fatal in case of severe intoxication. We report a case of a healthy 32-year-old woman who went to the local emergency department (ED) 30 min after ingesting, accidentally, 5000 mg of anhydrous caffeine for a preworkout supplement. At the ED, she presented an episode of presyncope followed by agitation. ECG showed polymorphic broad complex QRS tachycardia and arterial blood gas revealed metabolic acidaemia with severe hypokalemia. The dysrhythmia was successfully treated with intravenous propranolol. Acid–base and hydroelectrolytic disorders were also corrected. A persistent sinus tachycardia was observed in the first 2 days in the ward and 5 days later she was discharged asymptomatic with internal medicine follow-up.
- poisoning
- vitamins and supplements
- arrhythmias
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
This case illustrates the life-threatening consequences, such as malignant cardiac arrhythmias, of severe caffeine poisoning, which is a rare event. Also, it highlights the risk of accidental caffeine overdose associated with sports practice, which can be related, not only, to the difficulty in measuring small portions, but also due to unclear consumer’s instructions.
Case presentation
A 32-year-old woman with no significant medical and family history presented to the local emergency department (ED) referring malaise, anxiety, dizziness and nausea. Symptoms like chest pain, syncope, palpitations or fever were denied.
The initial physical examination at triage revealed a Glasgow Coma Scale (GCS) of 15, a respiratory rate of 19 breaths/min, 100% oxygen saturation on room air, blood pressure of 112/70 mm Hg, pulse of 80 beats/min and had a normal tympanic temperature. Also, the blood sugar was 147 mg/dL.
After observation, the patient had an episode of presyncope followed by agitation and vomiting. At this point, the patient was pale and sweaty with a GCS of 11 (eye opening: 4; verbal response: 2; motor response: 5), blood pressure of 115/75 mm Hg, tachycardia (160 beats/min) and 99% oxygen saturation on room air. Her pupils were equally round and reactive to light, and no muscle weakness or sensory deficits were found.
The ECG showed a polymorphic broad QRS tachycardia and the arterial blood gas revealed metabolic acidaemia with severe hypokalemia. The dysrhythmia was successfully treated with 5 mg of propranolol intravenous in total. Acid–base and hydroelectrolytic disorders were also corrected.
After stabilisation, the patient informed the ED’s physician that when she was preparing the preworkout supplement, used the same dosage of the proteic supplement for anhydrous caffeine, instead of 1 dose of 300 mg (6 mg/kg) of anhydrous caffeine, the patient consumed a total of 5000 mg (89 mg/kg), 30 min before going to the ED. The patient switched the dose dispensers shown in figure 1.

Two view angle of dose dispensers; (A) dose dispenser for the proteic supplement; (B) dose dispenser for the anhydrous caffeine.
The patient’s body weight was 56 kg. The patient also indicated that she occasionally drinks one espresso (60 mg of caffeine) and has never used alcohol or any recreational drugs.
Investigations
The initial group of complementary exams was:
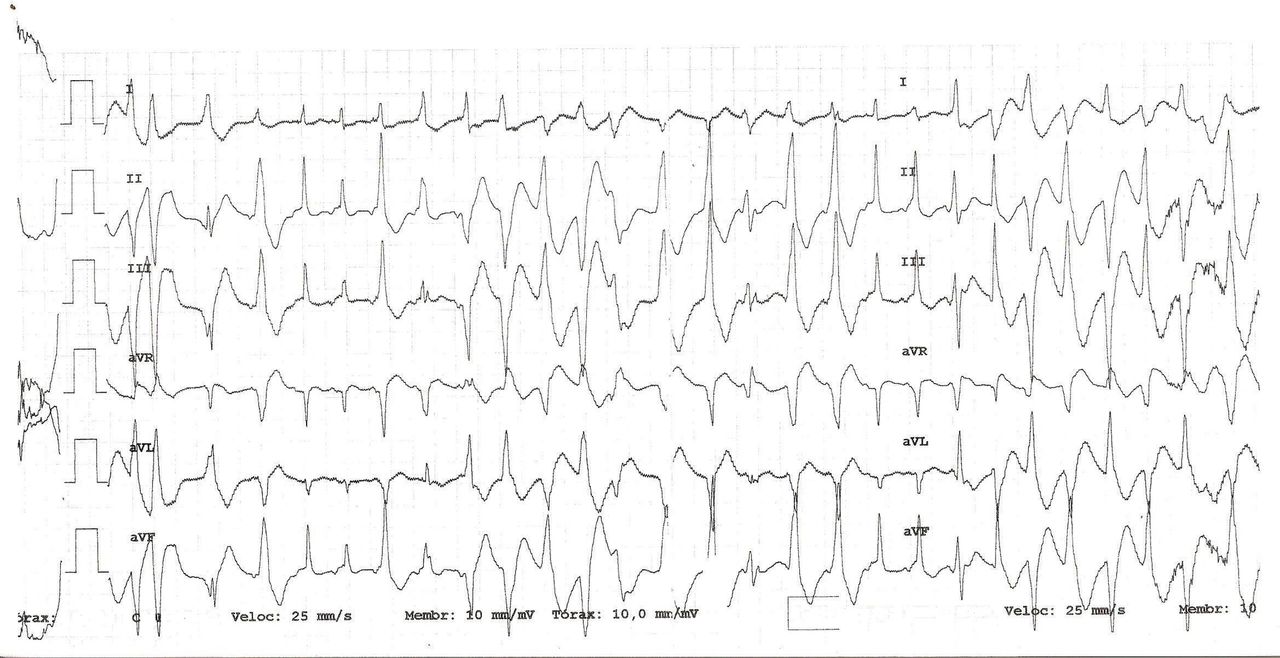
Electrocardiogram (figures 2 and 3) showing a broad QRS polymorphic tachycardia.
Arterial blood gas showed a metabolic acidosis with pH of 7.296 (7.35–7.45), pCO2 of 29.9 mm Hg, pO2 of 117 mm Hg, HCO3 of 16.1 mmol/L (22–26) and severe lactataemia with serum lactate level of 5.3 mmol/L (0.5–1.6).
Prominent laboratory findings included mild leucocytosis of 13.50×109/l (4.0–10.0) with 68.3% neutrophils, hyperglycaemia of 254 mg/dL (70–105), hypocalcaemia of 2.5 mmol/L (3.5–5.1) and hypophosphataemia of 1.8 mg/dL (2.3–4.7). Magnesium and calcium serum values were within normal range as well as thyroid, renal and liver function tests.
Urinalysis was positive for ketones and glucose and negative for cocaine and opioid drugs. Unfortunately, a blood sample for caffeine analysis was not taken.
Plain chest X-ray was normal.
Echocardiogram revealed a structurally normal heart.
The supportive treatment, including intravenous fluids, propranolol, potassium and phosphorus supplementations, stabilised the patient’s clinical status. No activated charcoal was administered as the medical team was unaware of a dietary product ingestion during the initial evaluation. After 48 hours of observation in our intermediate care unit, the patient was transferred to the ward, since she only had a asymptomatic sinus tachycardia (maximum of 120 beats/min), with other vital signs remaining stable and normal serum pH, lactate and glucose levels.
Case study limitations
A blood sample to assess caffeine’s level was not taken.
The dietary product ingested was not submitted to chemical analysis to assess quantitative caffeine’s level.

ECG showing a broad QRS polymorphic tachycardia.
{kind=link}
{kind=link}
{kind=link}
Rhythm strip showing a broad QRS polymorphic tachycardia.
Outcome and follow-up
The patient remained in our intermediate care unit for 2 days, with normal level of consciousness maintained, normalisation of arterial blood gas values and no recurrence of presyncope episodes.
However, she had persistent sinus tachycardia and, for this reason, was submitted to a 3-day course of 30 mg/day oral propranolol with heart rate control. The patient remained clinically stable and 5 days later was discharged asymptomatic referred to internal medicine follow-up.
The patient performed a treadmill exercise stress test by Bruce Protocol with adequate chronotropic response, normotensive profile and negative result for myocardial ischaemia.
Six months after the episode, at follow-up evaluation, the patient remained asymptomatic.
Discussion
Caffeine (1,3,7-trimethylxanthine) is a natural product commonly found in foodstuffs, beverages and medicinal products.1
When relatively low doses of caffeine are consumed, severe side effects are uncommon.
However, in recent years, larger amounts of caffeine have been added to energy drinks or taken as dietary supplements, such as anhydrous caffeine, for increasing endurance, concentration and athletic performance.2 3
Normally, mild stimulation is obtained with a caffeine dosage of 0.05–0.2 g. Even though fatal caffeine intoxication is rare, acute ingestion of >5 g can be lethal.4 5
After oral intake, around 90% of the product is rapidly absorbed from the gastrointestinal tract and clinical effects are observed within 15 min with a peak effect within 1–1.5 hour after consumption.1–3 Half-life elimination of caffeine varies between 3 and 7 hours and has several modifying factors such as sex, age, use of oral contraceptives, pregnancy and smoking.1
Therefore, there is a significant variability regarding ingested amounts and their toxic effects.6
Caffeine is structurally similar to adenosine and acts as a competitive antagonist on adenosine receptors.1 3 7 8 Adenosine receptors are found throughout the human body. However, they have a specific role in the brain and heart.7 8
By blocking the adenosine receptors, at high doses, caffeine interacts with the sympathetic nervous system inducing prolonged and intensified beta-receptor activation with positive inotropic and chronotropic effects which can trigger arrhytmia.3 7 And in toxic doses, caffeine directly releases calcium from intracellular stores, which also may increase the susceptibility for arrhythmias.8
Symptoms of caffeine intoxication may include headache, fever, nausea, vomiting, tachycardia, dizziness, tinnitus, anxiety, irritability, insomnia and seizures.1 3 4 8 Toxic levels of caffeine are also associated with severe hypokalaemia, hyperglycaemia, rhabdomyolysis, renal failure and hyperlactacidaemia.6 8 Leucocytosis, mild metabolic acidosis, ketonuria, hypophosphataemia and hypocalcaemia have also been described.9
Common cardiovascular effects are described as hypertension followed by hypotension and cardiac dysrhythmias, including supraventricular and ventricular tachyarrhythmias.6 8
Arrhythmias are considered the most common cause of caffeine-related death.10
The determination of blood caffeine concentration might be useful in confirming the diagnosis.3 9 Nevertheless, it is not easily measured at most emergency departments and the magnitude of caffeine toxicity is clinically determined.7 9
Morita et al suggests that the plasma lactate concentration allows establishing the severity level of the caffeine intoxication. This phenomenon can be explained by the excessive sympathetic stimulation caused by caffeine overdose, and therefore, glycogenolysis and lipolysis are increased with a consequently pyruvate level raise. If pyruvate does not enter the aerobic pathway, it is converted to lactate instead, which causes hyperlactacidaemia.6
Treatment of caffeine toxicity can vary on case-to-case basis. However, it should begin with careful and immediate assessment of the patient’s airway, breathing and circulation. Not only should non-invasive monitoring, like continuous cardiac monitoring, and fingerstick glucose level be rapidly obtained, but also intravenous access must be established.9 11 12
To prevent systemic effects of the caffeine metabolism, activated charcoal and intravenous lipid emulsion can be useful interventions. To address hypotension, intravenous fluid therapy with isotonic fluid should be initiated.12
Any patient with a haemodynamically unstable dysrhythmia should be treated by advanced cardiac life support protocols.9
In several published case reports, a combination of a short-acting beta-blocker (eg, esmolol, propranolol), procainamide or lidocaine with electrolyte correction successfully treated cardiac arrhytmias.11 13 In certain cases, dialysis is also referred as a successful treatment for patients with caffeine toxicity.11
In conclusion, we describe a case of severe caffeine intoxication due to an accidental high dosage of this component as preworkout dietary supplement.
With the increasing popularity of anhydrous caffeine consumption for sport enhancing, the clinical awareness of caffeine toxicity should be increased. The high purity of product content, small serving size and unclear dosing instructions may be risk factors for unintentional consumption for toxic doses of caffeine.
Given that cardiac arrhythmias are the most frequent cause of death by caffeine overdose, sports practitioners should be informed on the potential health hazards related to excessive caffeine intake, as well as, dietary supplements should be better regulated and reported on food labels.
In the future, we suggest contacting the regional poison control centre to improve and increase dataset which can contribute to enhance federal analysis and the correct legislation of this kind of products.
Learning points
Caffeine overdose can be fatal.
Cardiac arrhythmia is a frequent consequence that needs immediate management.
Clinical awareness of caffeine toxicity should be increased.
Footnotes
Contributors AA, CS, MP and MF: contributed to the planning and conduct of this article. AA: collected, analysed and discussed, with MP, all data in this clinical case; prepared the manuscript draft with support from CS and MF, with critical feedback and helped organize the manuscript. AA and CS: analysed the review and rectified the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.