Article Text

Statistics from Altmetric.com
Description
A 44-year-old woman was diagnosed with corneal dystrophy (figure 1) and anaemia. Analytically, she showed an altered lipid profile (cholesterol 172 mg/dL, triglycerides 173 mg/dL, high-density lipoprotein (HDL) cholesterol 6.6 mg/dL, low-density lipoprotein cholesterol 131 mg/dL, very low-density lipoprotein (VLDL) cholesterol 45 mg/dL, VLDL triglycerides 143 mg/dL, apo A 62 mg/dL, apo B 69.6 mg/dL, lipoprotein A <2.5 mg/dL) and proteinuria between 1 and 2 g/day. A renal biopsy was performed. Histology revealed the presence of segmental hyaline lesions and irregular mesangial enlargement. Glomerular capillary walls showed parietal thickening and subendothelial deposits, vacuolisation and frequent images of reduplication of the basement membrane (figure 2). Electron microscopy showed lipid deposition in many areas (figure 3). The evaluation of the plasma lecithin cholesterol acyltransferase (LCAT) enzymatic activity was 15.2 nmol/mL/hour (reference range, 81±12 mL/min/hour). A genetic study of LCAT deficiency disease was performed which showed a missense homozygosis in the LCAT gene c368G>Cp (R123p), not previously described in literature.

Slit lamp image of eye demonstrating corneal opacification. Cornea shows generalised haziness in stromal layer with accentuation at the periphery forming a circumferential corneal arcus.
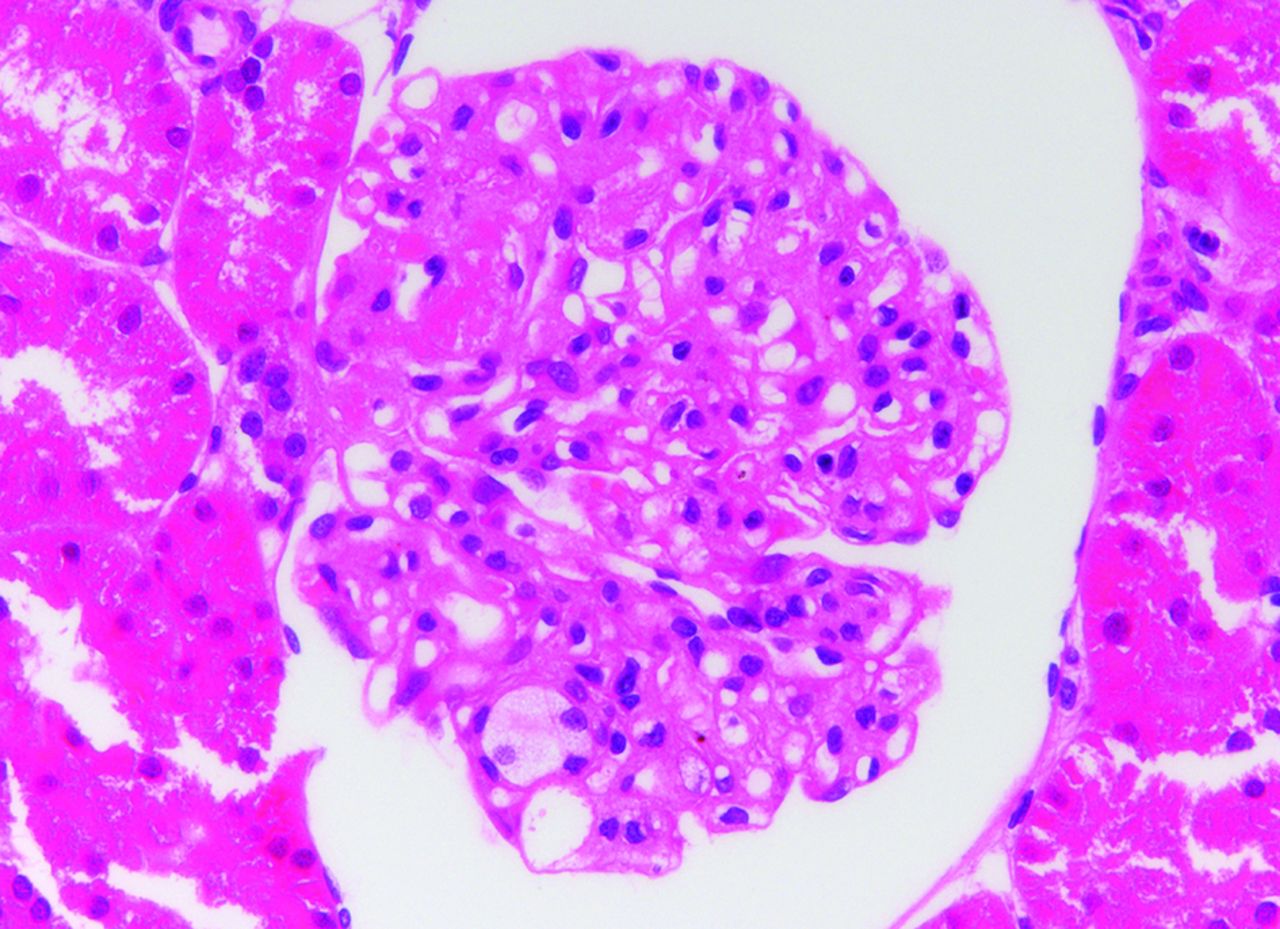
H&E shows mesangial expansion, thickening of the capillary walls and foam cells filling the capillary lumina.
{kind=link}
{kind=link}
{kind=link}
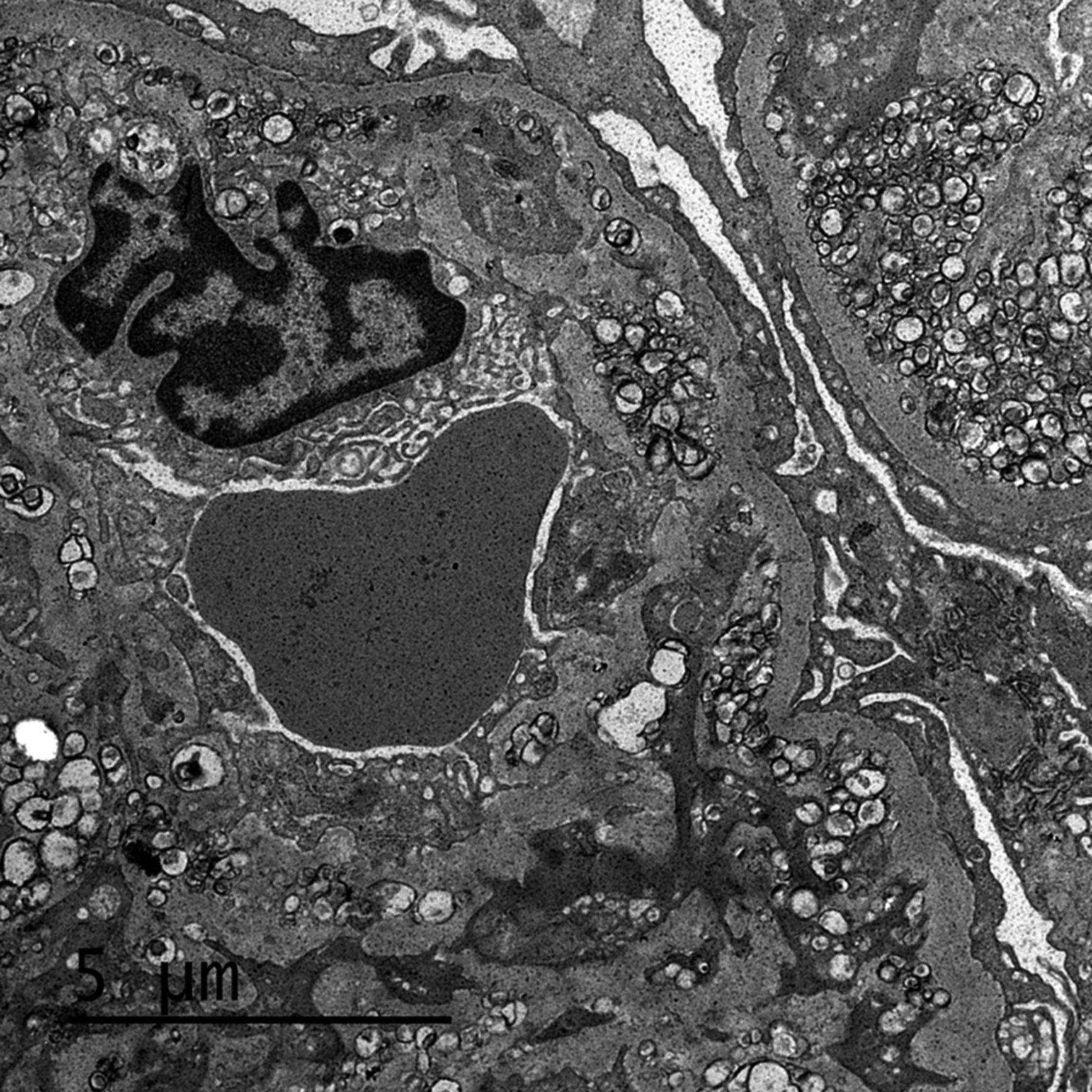
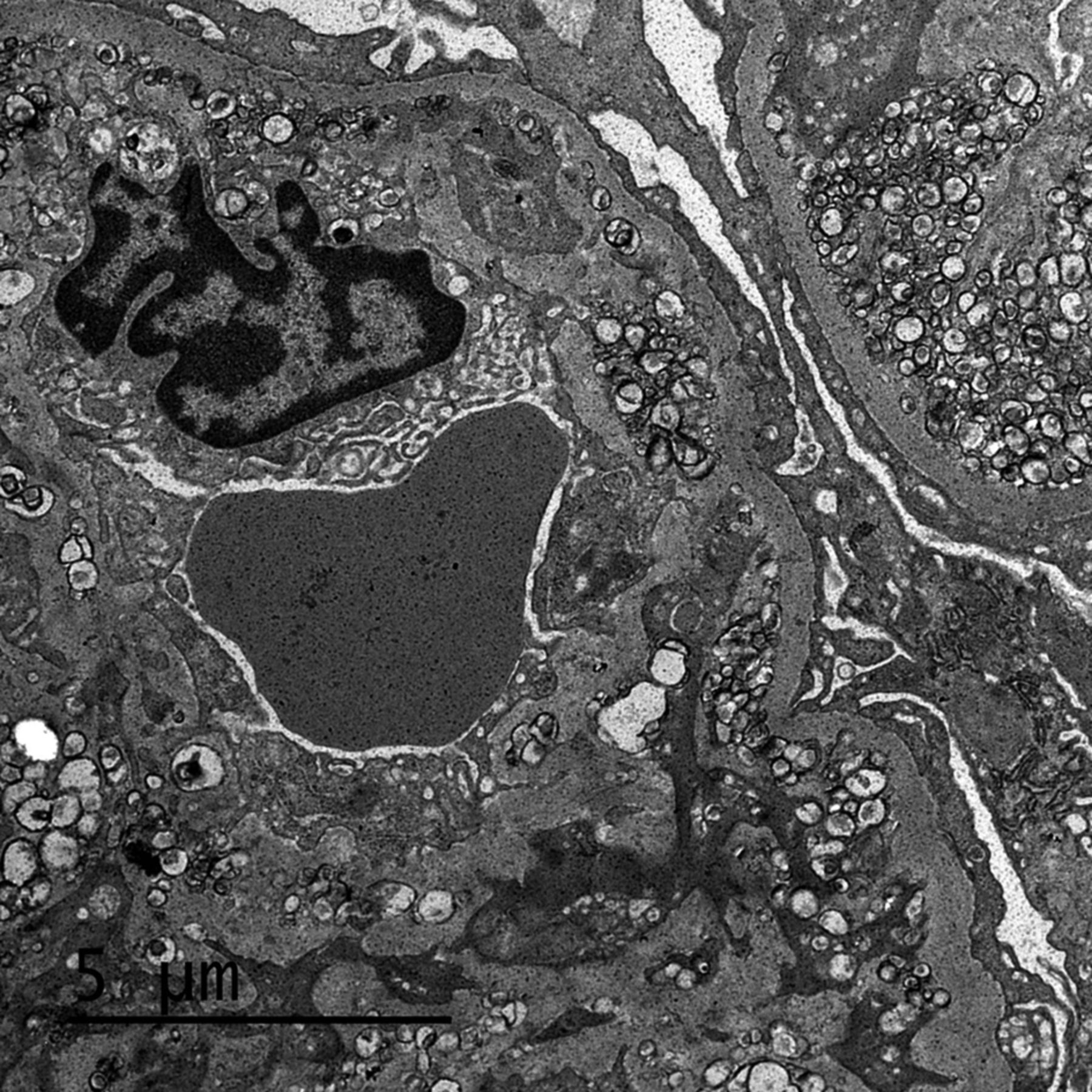
Electron microscopy shows subendothelial, intramembranous and mesangial electron-dense, rounded lamellar deposits.
Complete LCAT deficiency disorder is a very rare condition with an incidence rate of less than 1 in 1 million individuals. This disorder is caused by a mutation in the LCAT gene. The LCAT gene encodes the enzyme LCAT, which binds blood and tissue cholesterol to lipoproteins in order to transport it to the liver.1 The signs and symptoms include corneal opacification, haemolytic anaemia and proteinuria. Kidney disease is the major cause of morbidity in these patients. Hypertension and progressive deterioration of renal function leading to end-stage of renal disease are frequent and need renal replacement therapy.2 Characteristic analytical findings include an abnormal lipid profile with markedly decreased HDL cholesterol, apo A and apo B values and increased triglycerides.3 There is no established treatment for this entity; however, the infusion of recombinant human LCAT has been tried with favourable results: improvement of anaemia, normalisation of HDL cholesterol and slowing progression of chronic kidney disease.
Learning points
Lecithin cholesterol acyltransferase (LCAT) deficiency disorder is an extremely rare genetic disorder.
The patients with LCAT deficiency have an abnormal lipid profile (very low levels of high-density lipoprotein cholesterol, apo A1 and apo B).
LCAT deficiency disorder includes proteinuria and progressive chronic kidney disease and fat deposits in the corneas of the eyes.
Footnotes
EM and MM contributed equally.
Contributors EM: drafting the article or revising it critically for important intellectual content. MA and BS: conception and design, acquisition of data, or analysis and interpretation of data. MM: final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.