Article Text

Statistics from Altmetric.com
- urinary and genital tract disorders
- general practice / family medicine
- tropical medicine (infectious disease)
- tropical medicine
- general surgery
Description
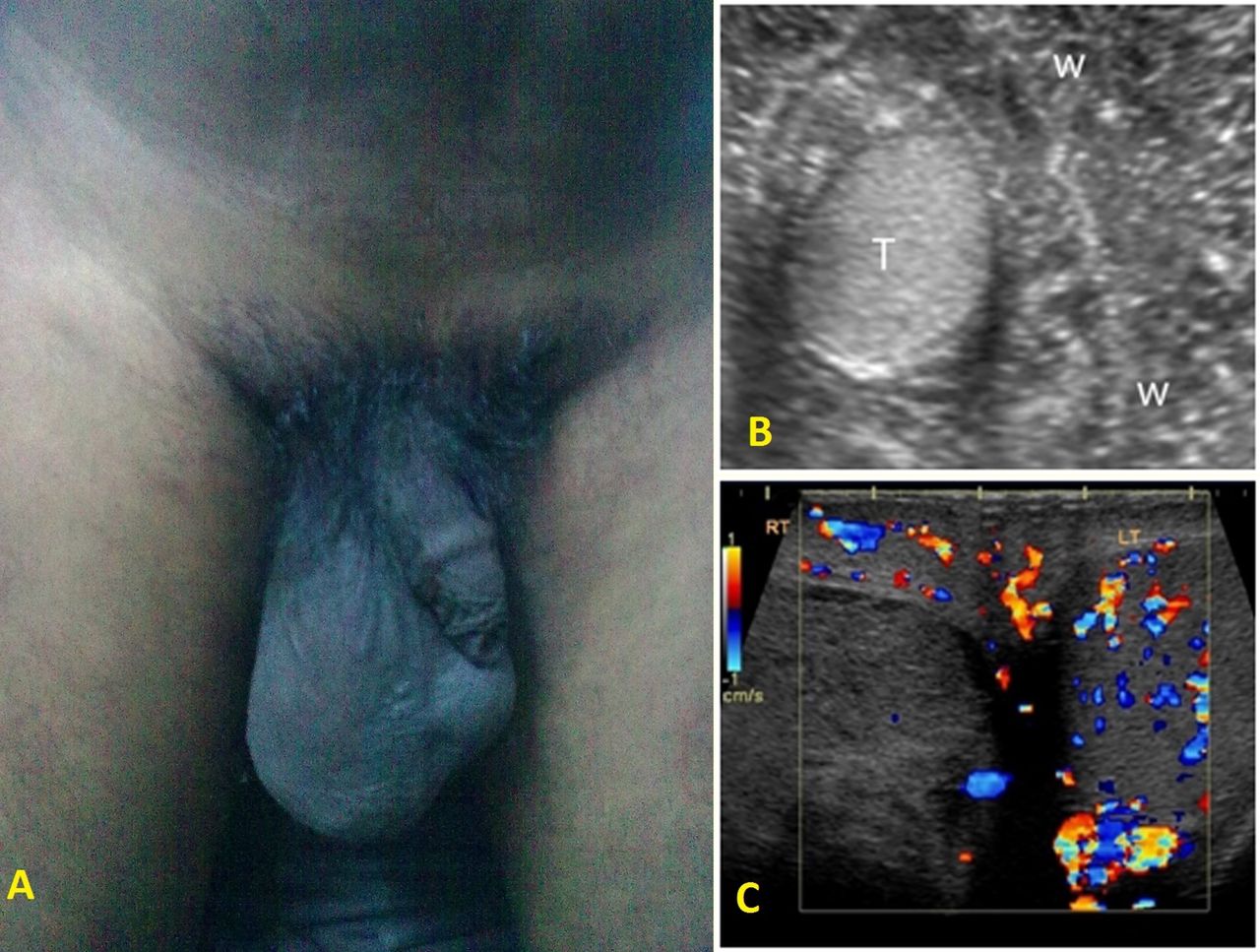
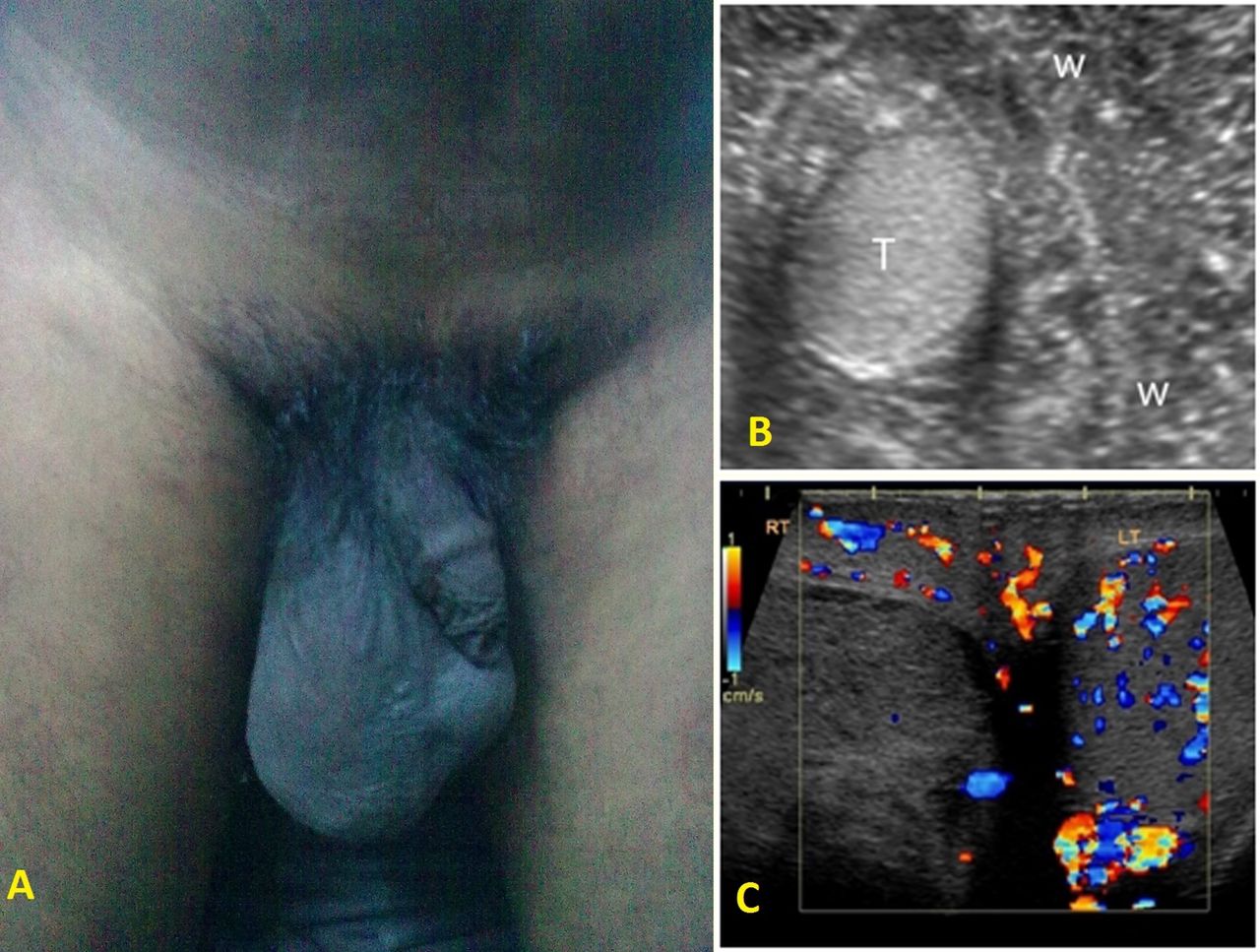
A 33-year-old man presented with recurrent pain and swelling in the inguinal region since the last 8 years, occasional fever and loss of sex drive. The pain and swelling usually lasted for 2–3 weeks with a pain-free interval of 4–5 months. He felt that the size of the left testis is gradually reducing. He had been married for more than 5 years without having any children. Clinical examination revealed swelling and tenderness of the scrotum more on the right (figure 1A).
{kind=link}
(A) A 33-year- old man with right-sided testicular swelling. (B) Ultrasonography of the scrotum reveals a hypoechogenic, small right testis with irregularly echogenicity in periphery due to fibrosis. (C) Colour Doppler reveals absence of vascular flow on right-side testis.
Ultrasound examination showed swelling of both epididymis with the outer area appearing irregularly echogenic due to fibrosis (figure 1B). The right cord appeared swollen and measured 8.75 mm, normal being below 5 mm. A colour Doppler study revealed absence of vascular flow on the right side testis (figure 1C).
Seminal fluid analysis was done. The total sperm count was 9.4 million/mL having low viscosity with non-motile dead spermatozoa about 40%. The circulating adult filarial antigen test (OG4C3) was positive (512 antigen units). OG4C3 test is a highly sensitive and specific quantitative monoclonal antibody-based ELISA test for the diagnosis of filariasis.
A diagnosis of right filarial funiculitis with bilateral chronic epididymitis and secondary infertility was made. The patient was treated with amoxicillin and clavulanic acid 2 g daily, orally for 1 week, along with a course of diethylcarbamazine for 2 weeks as recommended by WHO guidelines. Flavonoid supplements were added for 2 weeks to reduce inflammation and pain. Following therapy, the patient had symptomatic relief of pain and fever, with reduction in swelling over right testis over a period of 6 months. A repeat seminal fluid analysis after 6 months however revealed a marginal improvement in sperm count (10 million/mL).
Lymphatic filariasis, most commonly due to Wuchereria bancrofti, is responsible for affecting nearly 120 million people worldwide and disfiguring another 40 million people.1 The adult filarial worm resides in the lymphatic system and disturbs the normal lymphatic function. Genital manifestations of lymphatic filariasis in men include hydrocele, lymphorea, epididymo-orchitis, ram horn penis and infertility.2 The exact mechanism of infertility in filariasis is unknown. Frequent epididymal inflammation and scarring leading to blockage of tubules may cause obstructive azoospermia. Development of antispermatozoa antibodies may also be a cause.3
This manuscript highlights the devastating complication of infertility that may occur in untreated or late-treated bancroftian filariasis.
Learning points
Lymphatic filariasis may present with numerous genital manifestations resulting in disfigurement and psychosexual abnormalities.
Secondary infertility may be an incapacitating and devastating outcome of genital involvement in lymphatic filariasis.
Lymphatic filariasis should be considered strongly as a differential diagnosis in patients with genital inflammation and swelling in endemic areas.
Footnotes
Contributors DKP and DPM were involved in literature review and manuscript preparation. Both authors have evaluated the final manuscript before submission.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.