Article Text

Statistics from Altmetric.com
Description
We present three patients, treated at our intensive care unit (ICU), with radiological signs of free gas in different tissues.
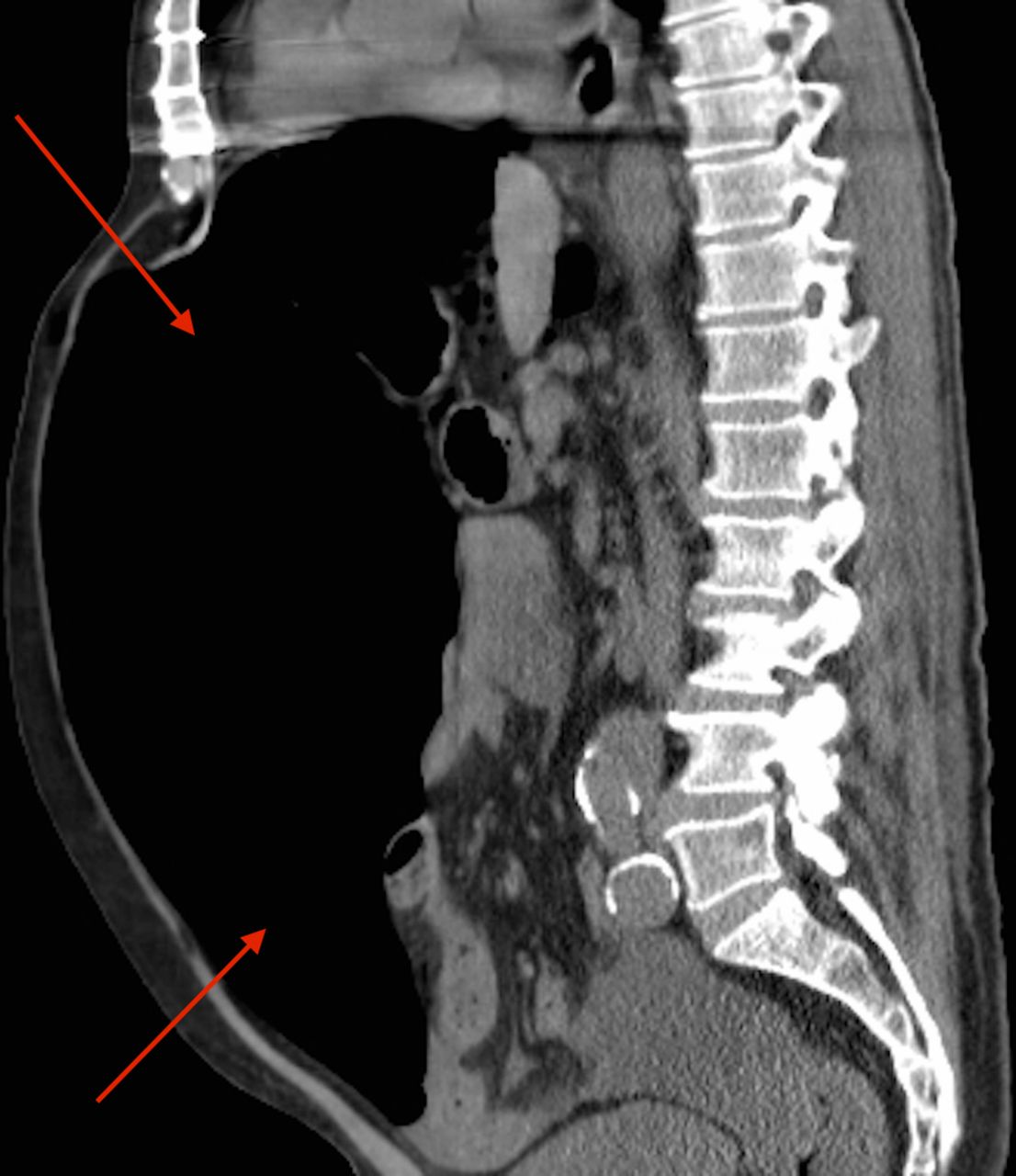
Patient A, a 67-year-old man with a history of colitis ulcerosa, was admitted with acute right upper quadrant pain and fever. An abdominal X-ray (figure 1) showed free gas under the diaphragm and Rigler’s sign (indicating the presence of gas on both sides of the bowel wall).1 The CT scan revealed a toxic megacolon with signs of a pneumoperitoneum (figure 2) caused by a colon perforation.

Free gas in the abdominal cavity and Rigler’s sign (indicated by white arrows).

A toxic megacolon with signs of a pneumoperitoneum (indicated by red arrows).
Patient B, a healthy 62-year-old man, presented with malaise and substernal chest pain. During physical examination, a retropharyngeal abscess was found. The CT scan revealed an extensive pneumomediastinum with gas penetrating into the nuchal region (figure 3). Both patients showed signs of sepsis with tachypnoea, tachycardia and fever.

An extensive pneumomediastinum and gas penetrating into the nuchal region (indicated by red arrows).
Patient C, a 78-year-old woman with Addison’s disease, complained of subacute fever and back pain. Her CT scan revealed a pneumomyosis and pneumovertebralis (respectively intramuscular and intravertebral gas) caused by a perforated diverticulitis with a fistula (figure 4). However, her vital signs were stable. Suppression of septic shock due to a maintenance dosage of prednisolone was therefore suspected.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pneumomyosis and pneumovertebralis (indicated by red arrows).
All patients were immediately treated with broad-spectrum antibiotics and underwent subsequent surgical exploration. Patients A and C had a pneumoperitoneum, indicating free gas trapped within the peritoneal cavity but outside the lumen of the bowel. Patient B had a pneumomediastinum due to mediastinitis. Afterwards, they were admitted to the ICU for postoperative care. Patients A and B both went into severe septic shock. Against all odds, patient C recovered without any clinical sequelae.
A complete summary of differential diagnoses regarding free gas can be found in table 1. Up to 49% of cases of a pneumoperitoneum may not be detected using conventional radiography. Therefore, it is recommended to make a CT scan, which can correctly identify the site of perforation in 86% of the cases.2 After taking microbiological cultures, broad-spectrum antibiotics should be started immediately if sepsis is suspected. However, there may also be causes of free gas for which antibiotics are not the direct course of treatment. Surgical exploration is mandatory if sepsis source control is required.
Differential diagnosis of free gas
Radiological images showing free gas are alarming as this may indicate a possible fulminant course of disease. In these cases, an initial aggressive approach is justified. Striking images of patients presenting with free gas, however, are not always concordant with a rapid disease progression. Therefore, the interpretation of clinical findings and radiological images should always be combined for appropriate decision-making.
In conclusion, due to the possible severe course of disease, every patient with free gas should be approached with caution. Depending on whether there is a suspicion of sepsis, immediate source control through explorative surgery and postoperative ICU care should be considered.
Learning points
Imaging showing free gas warrants a high index of suspicion; however, striking images are not always concordant with the course of the disease.
Free gas has different anatomical origins and not all causes are life threatening.
Sepsis as a cause requires antibiotic treatment and usually surgical source control.
Footnotes
NK contributed equally,
C contributed equally.
Contributors NvR participated in writing the article (and revision) and received informed consent from the patient. CS participated in writing the article (and revision). NvR, CS and DHTT were closely involved in patients’ stay at ICU. DHTT critically revised the article. NvR and CS are guarantors and contributed equally.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.