Article Text

Summary
Acute compartment syndrome (ACS) is a surgical emergency that requires urgent fasciotomy to prevent irreversible sequelae. We report two cases of unidentified ACS, which did not result from traumatic injuries such as fractures or crush injury, iatrogenic injury or diseases such as haematological malignancies. Both patients complained of severe pain and swelling of their extremity. No bite marks, blisters or skin necrosis was noted. They also complained of marked symptoms of third cranial nerve injury, including divergent squint and diplopia. The diagnosis of ACS was made following continuous intracompartmental pressure measurement, and both patients underwent urgent fasciotomy with partial incision. Considering the season and location of the injuries, together with the rapid progression of signs and symptoms that included thrombocytopaenia, acute renal failure, rhabdomyolysis and especially that of third cranial nerve injury, we postulate that these two cases may have developed following mamushi (Gloydiusblomhoffii) bites.
- orthopaedic and trauma surgery
- emergency medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Acute compartment syndrome (ACS) usually develops following traumatic injuries to the extremity such as fractures or crush injury. Occasionally, it may also occur as a result of a relatively minor injury, iatrogenic injury or secondary to diseases such as haematological malignancies.1–4
Regardless of the cause, ACS is a surgical emergency that requires urgent fasciotomy to prevent irreversible sequelae, as pressure that is not quickly relieved may lead to necrosis of the soft tissues and permanent disability.3 The irreversible functional loss of muscles usually occurs within 4 to 12 hours.5 We herein report two cases of unidentified severe swelling of the whole extremity resulting in ACS.
Case presentation 1
In April 2016, a 38-year-old man with no medical history presented to the emergency department complaining of severe pain of his left upper extremity. Eight hours prior to presentation, he sustained a fall in his backyard and noticed swelling over his left forearm with tolerable pain. X-ray and enhanced CT performed at the nearest hospital showed no evidence of fracture and/or internal haemorrhage of his forearm. He was subsequently referred to our institution for suspected ACS when his pain and swelling progressed. On first examination in our institution, his left forearm was markedly swollen, with extension to the left shoulder. He complained of severe pain as well as marked divergent squint and diplopia.
Investigations
There was no evidence of bite marks, blisters or skin necrosis (figure 1A). His white cell count was 11.5×109/L, while his creatine kinase (CK) level was 758 IU/L. There was thrombocytopaenia, elevated liver transaminases, elevated C reaction protein (CRP) level as well as coagulopathy and renal dysfunction. Urgent continuous intracompartmental pressure (ICP) measurement was performed with a slit catheter; the ICP within the flexor compartment of the left forearm was 55 mm Hg.

Case 1. (A) The left forearm was extremely swollen and extended to the left shoulder. (B) An urgent fasciotomy with partial incision of the left forearm was performed.
Emergent MRI was performed to confirm the presence of segmental lesion and to assess the range for fasciotomy during preoperative preparation right after ICP monitoring. MRI was efficient to identify the distribution and extent of muscle damage especially because both cases were unidentified. It showed oedema of the subcutaneous tissue and flexor muscle compartments (figure 2A).
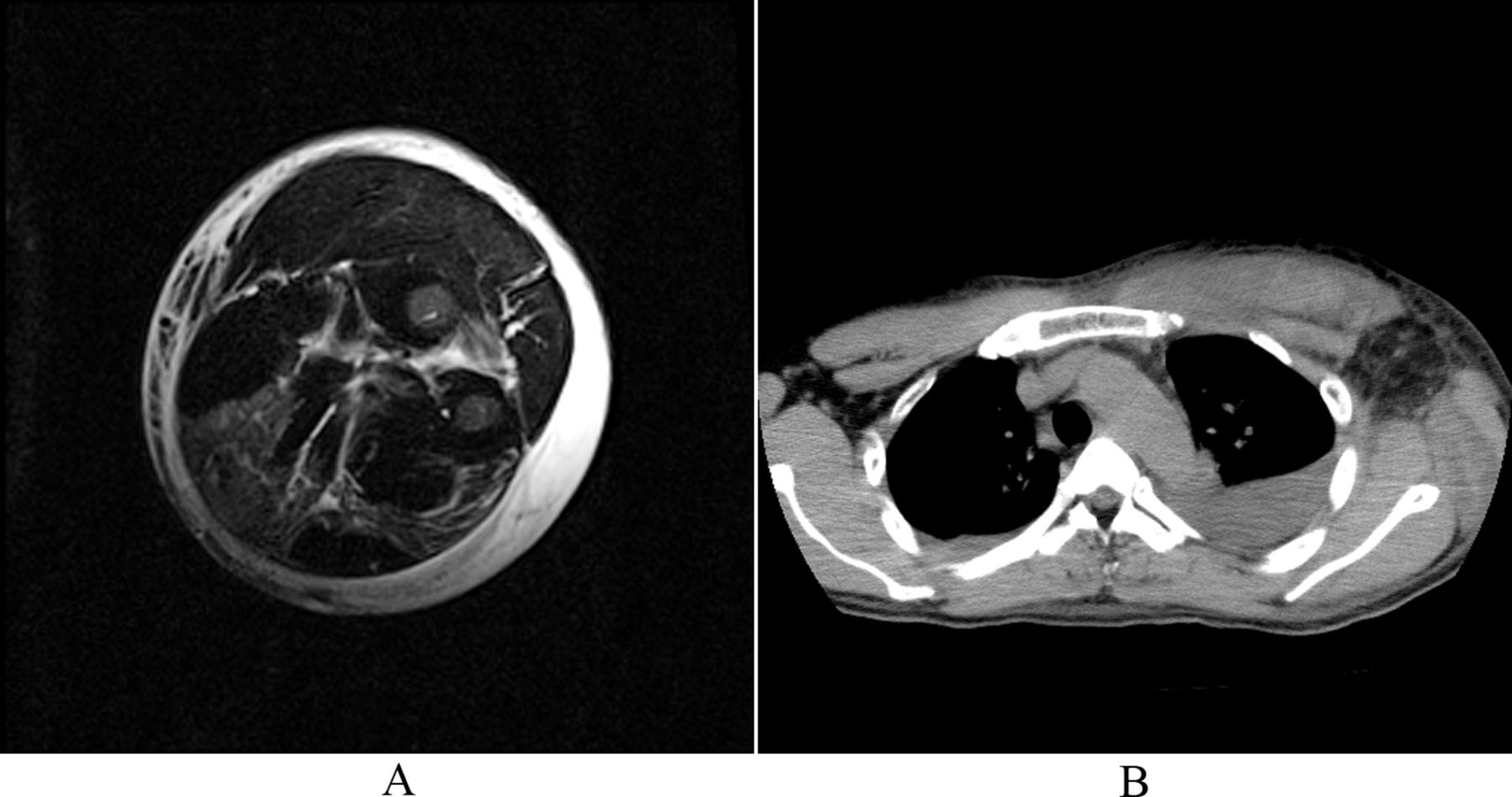
(A) MRI of the forearm showing oedema of the subcutaneous tissue and flexor muscle compartments. (B) CT showing left pleural effusion and severe oedema of the precordium.
Differential diagnosis
Acute compartment syndrome, unknown cause.
Treatment
In view of the rapidly progressive symptoms, we started the patient on high-dose clindamycin 2400 mg/day and sulbactam/ampicillin (SBT/ABPC) 9 g. Intravenous Ringer’s lactate solution was also initiated. Ten hours postinjury (2 hours after arrival at our hospital), the patient underwent an urgent fasciotomy with partial incision in the flexor compartment, under axillary block anaesthesia (figure 1B). The presence of clear, serous and odourless exudate from the subcutaneous tissue was noted intraoperatively; there was no necrotising soft tissue. Following compartment pressure release, the ICP of the flexor compartment reduced to 28 mm Hg, whereas the extensor and lateral compartments’ ICP measured 22 mm Hg and 24 mm Hg, respectively.
Outcome and follow-up
On day 2 of admission, the patient developed left pleural effusion and severe oedema of the precordium, as evidenced on CT scan (figure 2B). The high-dose antibiotic therapy was discontinued on day 3 of admission in view of negative blood and exudate culture results. However, SBT/ABPC 1.5 g/day was initiated for 2 weeks as prophylaxis against secondary infection. Twenty-four hours following admission, the patient’s CK, aspartate transaminase (AST), alanine transaminase (ALT) and lactate dehydrogenase (LDH) levels progressively increased, up to a maximum of 199 100 IU/L, 2419 IU/L, 640 IU/L and 5508 IU/L, respectively, on day 3 (figure 3). These values subsequently normalised within 3 weeks. Urinary myoglobin level was also increased above 1.2×106 ng/mL. Thrombocytopaenia started on day 2 until the platelet level reached a minimum of 9.5×104/μL on day 6 before returning normal on day 9.
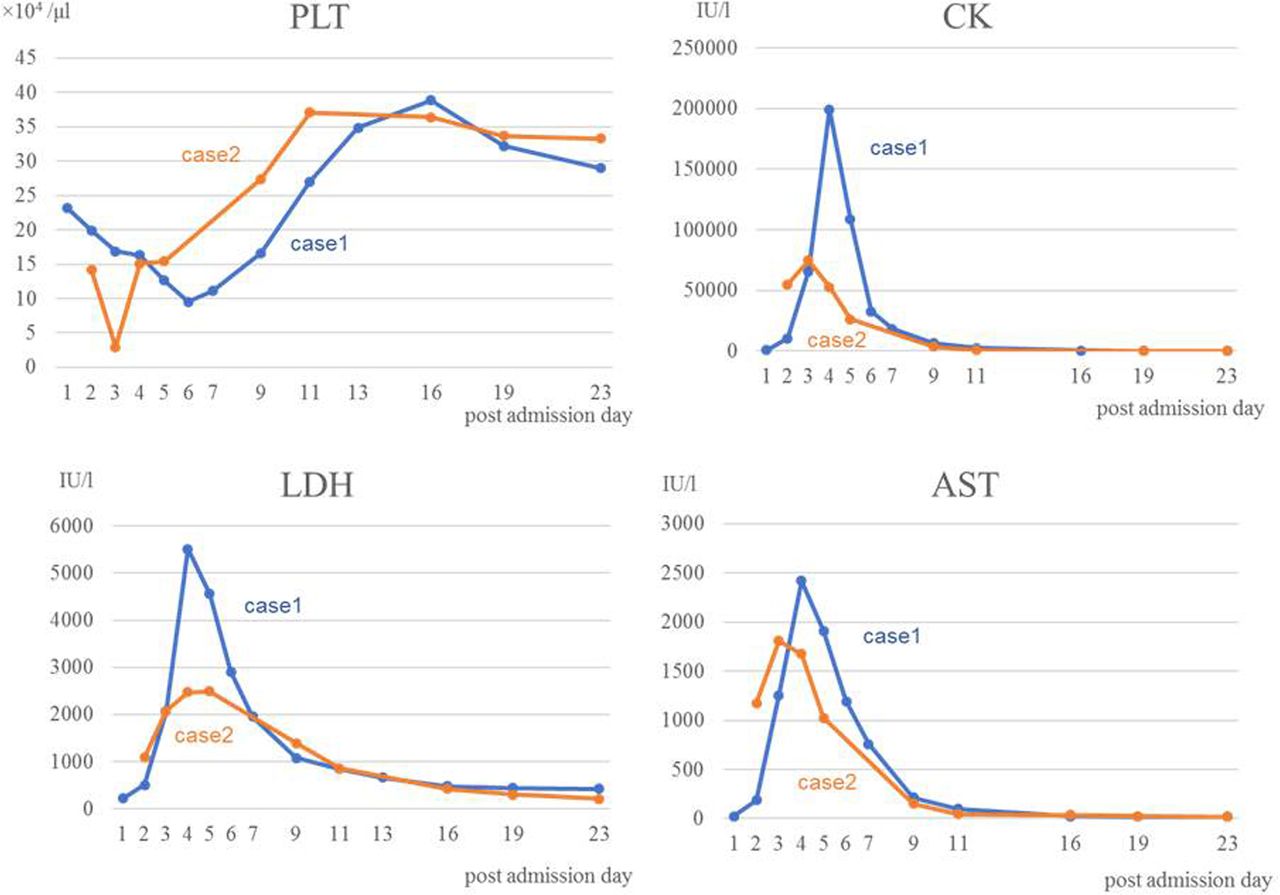
These panels show the laboratory results of PLT, CK,LDH and AST. AST, aspartate aminotransferase; CK, creatine kinase; LDH, lactate dehydrogenase; PLT, platelet.
Plasma fibrinogen level was 213 mg/dL on day 1, and this value did not change significantly. The patient also exhibited laboratory evidence of acute renal failure; from day 2, the blood urea nitrogen (BUN) and creatinine (Cre) levels gradually increased. On day 4 of admission, he was initiated on haemodialysis in view of worsening of BUN/Cre value, persistent oliguria despite receiving intravenous fluids and elevated CK. The BUN and Cre reached a maximum of 51 mg/dL and Cre 2.97 mg/dL, respectively, on day 10. Adequate urine output was regained on day 16, and haemodialysis was discontinued. The BUN/Cre value finally normalised after 2 months. The symptoms of third cranial nerve injury disappeared on day 4. Hand physiotherapy commenced on day 6, with a controlled active movement regimen. The fasciotomy wounds were closed with no skin graft on day 17 (secondary wound closure). The patient was discharged from the hospital with normal function of his left arm and hand on day 32. Full range of movement of the wrist and fingers, normal grip strength and normal sensation were present at clinical review 3 months postinjury.
Case presentation 2
In July2008, a 42-year-old man with underlying hyperlipidaemia was referred to our institution complaining of severe pain and swelling of his right lower extremity. Eighteen hours before presentation, he had tumbled down the street gutter and had consulted another hospital. He was initially treated with antibiotics but was subsequently referred to us for suspected necrotising soft tissue infection.
Investigations
At the initial examination, the patient’s right lower extremity was markedly swollen, and he was in severe pain (figure 4). ICP of the four compartments (anterior, lateral, posterior-superficial and posterior-deep) of the right leg ranged between 110 and 140 mm Hg. MRI showed gross oedema of the subcutaneous tissue from the right gluteal region to the right foot (figure 5A,B). Laboratory investigation revealed a white cell count of 17.0×109/L, platelet of 14.2×103/μL, CK of 54 840 IU/L, AST of 1174 IU/L, ALT 269 of IU/L, LDH of 1086 IU/L and CRP of 5.41 m/dL. Urinary myoglobin level was elevated above 3000 ng/mL.

The right lower extremity with notable swelling.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI showing remarkable oedema of the subcutaneous tissue at the right femoral region (A) and the right cruris region (B).
Differential diagnosis
Acute compartment syndrome, unknown cause.
Treatment
Twenty hours postinjury (2 hours after arrival at our hospital), the patient underwent urgent compartment release with partial incision over the lateral and medial sides of the leg, under lumbar anaesthesia. Intraoperative finding revealed clear, serous and odourless exudate; no necrotising soft tissue was observed.
Outcome and follow-up
Following compartment release, the ICP decreased below 30 mm Hg. Meropenem 1.5 g/day that was initiated prior to admission to our centre was discontinued 3 days after surgery in view of negative blood and exudate cultures. On day 2, the patient developed severe thrombocytopaenia (platelet 2.9×104/μL), which required platelet transfusion. After day 3, the platelet level maintained above 15.0×104/μL. Plasma fibrinogen level was measured at 335 mg/dL on day 2, and this value did not change significantly. His CK and AST reached a maximum of 74 701 IU/L and 1809 IU/L on day 2, but decreased to 215 IU/L and 23 IU/L, respectively on day 19 (figure 3). The symptoms of third cranial nerve injury disappeared within 1 week. The surgical incision wounds were sutured on day 17.
The patient continued to show clinical improvement without complications of peroneal nerve paralysis and was discharged home on day 48. After 2 years, his paralysis recovered completely.
Discussion
ACS is a surgical emergency that requires prompt diagnosis to prevent permanent tissue necrosis. Diagnosis is primarily based on clinical suspicion, as was demonstrated in the present two cases.1 ACS is commonly associated with high-energy injuries, such as fractures and soft tissue injuries.6 7 Our two cases were interesting in that they did not exhibit any of these injuries radiographically and intraoperatively. As ACS can occur in a variety of clinical situations and in various anatomical locations, we also excluded the possibility of external compression, such as circumferential cast or dressing, military antishock trousers and internal compression such as iatrogenic injuries, haematological malignancies, deep venous thrombosis or systematic capillary leak syndrome; these judgements were made based on the patients’ clinical and medical history.6 8 9 There have been several reports of idiopathic ACS; however, none of them were associated with diplopia and exotropia.6 10 11 We postulate that these two cases may have occurred secondary to venomous bites/stings of animals such as snakes, insects, Latrodectus hasseltii, centipedes or wasps, all of which are found widely in Japan. However, of note, both the patients did not have any evidence of bite or sting marks. With the exception of a case of snake bite and several paediatric case reports of wasp stings, there are no reports of ACS induced by all the aforementioned creatures.12–14 Post-snake bite ACS is rare, and the incidence is below 6.6% in the current study.12 In addition, symptoms of third cranial nerve injury were previously reported in the case of postsnake bite ACS.15
Taking into account the season and time of injury, location of injury, rapid progression of symptoms, thrombocytopaenia, acute renal failure, rhabdomyolysis and diplopia and/or exotropia, we postulate that the two cases described herein were atraumatic ACS secondary to mamushi (Gloydius blomhoffii) bite.1–4 15 16 However, a diagnosis could not be established owing to the lack of bite marks and clinical history of bite.
Mamushi, a venomous pit viper, is widely found in Japan and is associated with frequent incidence of bites.15 17 18 Its venom causes severe swelling which compresses peripheral arteries and/or lead to ACS of the extremities. This may progress to hypovolaemic shock, renal failure and/or cardiovascular disorders.15 16 19 It is difficult to encounter mamushi even in the daytime, because of their small size (less than 60 cm in length). They also often hide in the grass and fallen leaves. Patients usually feel only a minor pain, similar to that of an insect bite or splinter, because the mamushi fangs are only approximately 5 mm long and are very thin. As small bite marks may be difficult to observe, diagnosis by bite marks alone is almost impossible to make.15 18 The mamushi venom contains a small amount of neurotoxin, which causes diplopia, blurry vision and exotropia, owing to action on the third cranial nerve. These symptoms remit within several days to approximately 2 weeks.15
In terms of thrombocytopaenia, the platelet level of patient 2 decreased significantly (2.9×104/μL) on day 2 in comparison with patient 1 (9.5×104/μL) on day 6. We believe that this difference may be attributed to whether the venom was directly injected into the blood vessel or not. If the venom was directly injected into the blood vessel, the platelet count would rapidly decrease to <1.0×104/μL within 1 hour of the bite.15
In both cases, the patients’ liver transaminase levels increased 1 day post injury. We believe that this was attributed to rhabdomyolysis same as high levels of urine myoglobin. High CK and myoglobin levels also indicate an increased risk for kidney damage and failure, as seen in patient 1.15 18
The interval between injury and compartment release was 10 hours in patient 1 (8 hours until presentation and 2 hours in the emergency room) and 20 hours in patient 2 (18 and 2 hours, respectively). Patient 2 developed temporary peroneal nerve paralysis, and we believe that this difference of 10 hours may have contributed to the increased risk of complications. Snake venom is composed of a chemically complex mixture that forms enzymatically active proteins after being injected into the human body. After the deposition of venom into the subcutaneous tissue, a poison-induced capillary leak may induce extravasation of plasma and erythrocytes, resulting in oedema and ecchymosis.12 Urgent fasciotomy helps to wash out the venom from the bitten region by improving venous and lymphatic drainage, in addition to decompression of the subcutaneous and compartment pressure of the extremity.19
Our report highlights the need to keep in mind that swelling of the extremities can result in clinical emergency, taking into consideration the clinical history, such as location, season and time of injury.
Mamushi bites are classified according to grades; this is applied clinically to decide on the severity of injuries.15 20 In the current report, both patients 1 and 2 sustained grade 5 injury, the most severe. In general, grades 3–5 are classified as severe.15 20 21 Although antivenom is required for patients with severe mamushi bites, it is difficult to decide on its usage without a definite diagnosis, as antivenom side effects, such as anaphylaxis or serum sickness disease, may occur. Administration of the mamushi antivenom during the hyperacute phase might be able to shorten the duration of hospital stay.21
Patient’s perspective
(Case 1) On my admission, I was in a lot of pain and had severe swelling with unknown cause on my left arm. I am satisfied with the treatment I received from the medical team. I got back to my preinjury state completely 3 months after the injury.
(Case 2) On my admission, my right leg had been very painful and had notable swelling. I was pleased with the medical care I received from the hospital staff. Although I had a slight symptom of peroneal nerve paralysis for about 2 years after the treatment, I could still perform my daily activities.
Learning points
In Japan, unidentified acute compartment syndrome (ACS) associated with the symptoms of third cranial nerve injury (eg, diplopia, blurry vision, exotropia) may result from snake bites (especially mamushi bite).
Other characteristics of post-mamushi bite ACS include injury time (spring daytime and summer night), location of injury (backyard and street gutter), rapid progression of symptoms, thrombocytopaenia, acute renal failure and rhabdomyolysis.
It is essential to diagnose ACS promptly and perform urgent fasciotomy to prevent permanent tissue necrosis before investigating the primary cause of the ACS.
Footnotes
Contributors Drafting the article: ST. Revising it critically for important intellectual content: MT, AS. Final approval of the version to be submitted: HH.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.