Article Text

Summary
A retired woman with left ophthalmic shingles of over 2 years’ duration attended with bilateral vision loss and systemic upset. Acute retinal necrosis with detachment was detected on right fundus examination. Cataract in left eye precluded funduscopy. Ocular ultrasonography revealed fibrotic retinal detachment in the left eye. MRI brain and orbits also showed signals of retinal detachment. No abnormal MRI signal within the optic nerve or brain was found. Varicella zoster virus was detected in ocular aqueous and blood samples. High-dose intravenous acyclovir was administered. HIV test was positive with a very low CD4 count. Antiretroviral medications were prescribed. There was no recovery of vision. She was certified as blind, and social services were involved in seeking to provide alterations to her home in view of her severe disability. This case highlights the importance of suspecting HIV in patients with severe or chronic ophthalmic shingles. Images and implications for clinical practice are presented.
- Hiv / Aids
- ophthalmology
- retina
- sexual transmitted infections (viral)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Viral retinitis is a rapidly progressive condition that may involve the entire retina and lead to severe loss of vision. The aetiological agents include cytomegalovirus (CMV), varicella zoster virus (VZV), herpes simplex virus (HSV) and rarely Epstein-Barr virus (EBV). Acute retinal necrosis (ARN) may occur in immune-competent individuals and is characterised by confluent, peripheral, necrotising retinitis, peripheral occlusive arteritis and moderate-to-severe vitritis. Progressive outer retinal necrosis (PORN) usually occurs in immune-compromised patients and can lead to the rapid involvement of the peripheral and central retina by full thickness necrosis with severe loss of vision from retinal detachment (RD) and optic neuropathy. As viral retinitis is a rapidly progressive disease and loss of vision, including in the fellow eye is a high risk, early diagnosis and treatment are critical. We urge clinicians to consider this diagnosis in patients with ophthalmic shingles who present with new onset reduced vision. We advise ultrasound examination when media opacities obscure retinal examination. We present such a case with implications to improve patient safety and clinical care.
Case presentation
A retired woman who developed left-sided herpes zoster ophthalmicus (HZO) for 18 months prior was attending the corneal clinic for keratouveitis in the left eye for 7 months. She attended the routine corneal clinic appointment and offered new symptoms of a 4-week reduction of right vision. She had been admitted to hospital after sustaining a nasal fracture secondary to a mechanical fall 4 weeks prior to the routine ophthalmic outpatient visit. There was no other medical history. She was on oral acyclovir 800 mg daily for ophthalmic zoster and tramadol as needed and pregabalin 450 mg daily for postherpetic neuralgia and mirtazapine 15 mg at night.
Vision; no perception of light (NPL) in both eyes. At the prior routine ophthalmic visit, the right eye was normal, as was right visual acuity (VA). Anterior segment examination of right eye was unremarkable. Diffuse stromal corneal scaring with long-standing pigmented keratic precipitates and 360 degrees posterior synechiae was present in left eye. Funduscopy in the left eye was precluded by cataract. Funduscopy in the right eye was impaired by vitreous haze. Multiple areas of white retinal swelling in the posterior pole with macula involvement were apparent (figure 1) in the right eye. Obliterated arterioles with perivascular sheathing (Kyrieleis’ plaques)1 were detected (figures 1 and 2). Ultrasound showed bilateral RDs.
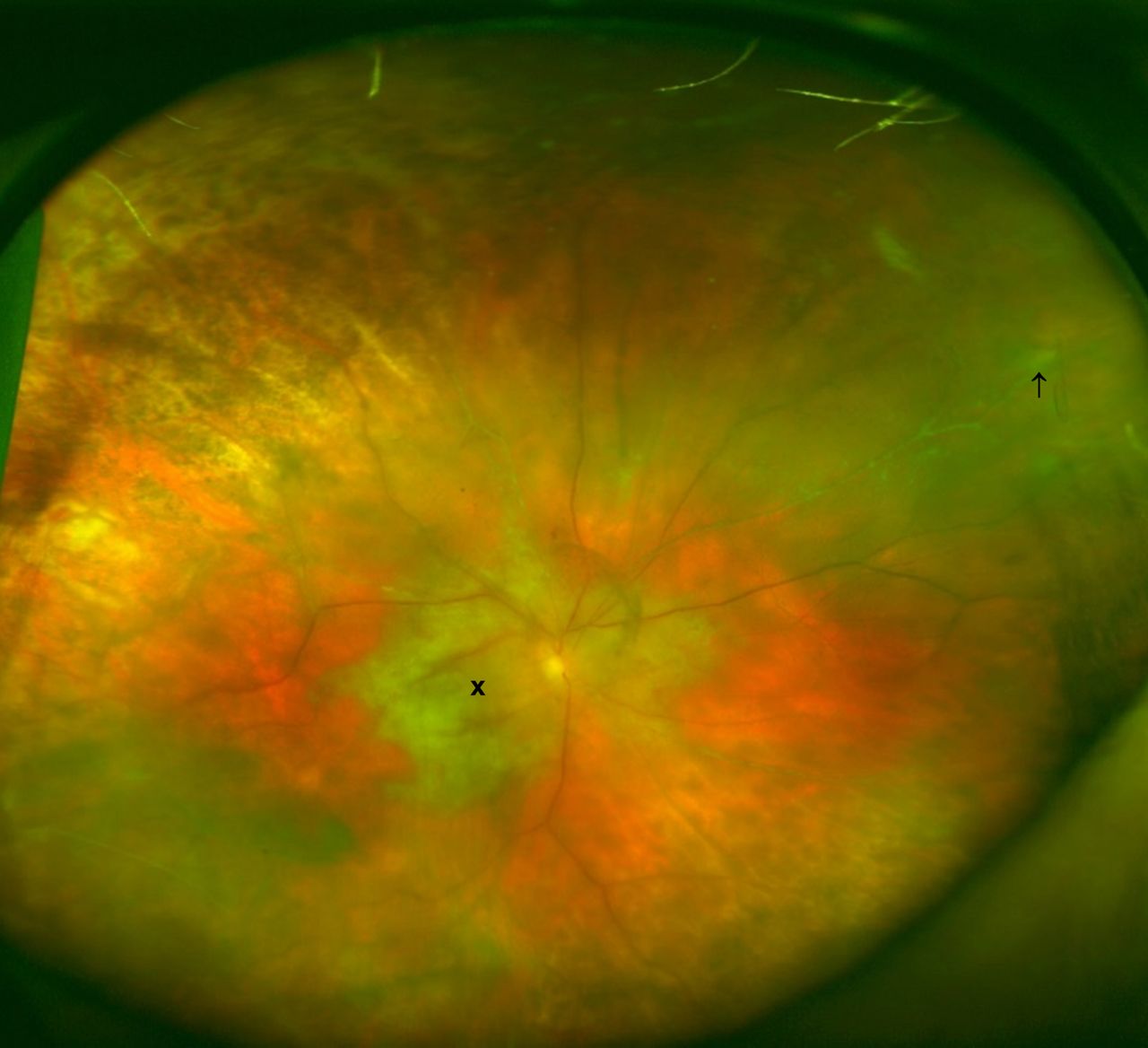
Widefield colour fundus image of the right eye. Centre (x) and peripheral (↑) involving retinitis.

{kind=link}
{kind=link}
Right eye: (A) Multicolour confocal scanning laser ophthalmoscopy (cSLO) image shows posterior pole retinal swelling in green and retinal arteriole thinning and periarterial focal Kyrieleis’ plaques (↑); (B) cSLO near-infra red reflectance image; focal, segmental and nodular periarterial plaques (↑) in the same locations.
Investigations
Haemoglobin 112 g/L, white cell count 3.1×109/L, liver function tests and urea and electrolytes were normal; C reactive protein 5.6 mg/L.
Blood cultures were negative for aerobic and anaerobic culture.
Toxoplasma and CMV serology negative, serum varicella zoster IgG positive, HIV positive, viral load was 116 912 copies/mL and CD4 T lymphocyte (CD4 cell) count was 37 cells/µL (normal value approximately 500–1300 cells/µL).
CMV DNA positive: 2308IU/mL in serum.
Aqueous from anterior chamber paracentesis of right eye was positive for VZV DNA on PCR and negative for CMV and herpes simplex.
Treatment
This patient was admitted to hospital and acyclovir 1.8 g daily by intravenous infusion was provided followed by oral valacyclovir 3 g per day. She received an intravitreal forscarnet injection (1.2 mg/0.05 mL).
Close liaison was undertaken with clinical microbiology and genitourinary medicine.
The HIV-positive result was discussed with the patient and antiretroviral therapy (ART) commenced. The patient revealed that she had engaged in unprotected heterosexual activity when travelling in Sub-Sahara Africa 5 years previously.
Outcome and follow-up
Following 1 week of ART, a repeat serum VZV DNA test was negative. Vision remains at NPL in both eyes. Bilateral RDs were considered as inoperable. The patient was registered blind and has had input from social services and community occupational therapy including modifications to her home because of acquired visual loss.
Discussion
Necrotising retinopathy may occur in patients with advanced HIV disease and is strongly associated with VZV infection.2 VZV, which is the most common aetiology, followed by HSV (types 1 and 2), CMV and EBV are other causative agents for necrotising retinopathy. It has been reported that PORN can also present as an initial manifestation of HIV.3
Our patient had vitreous inflammation with peripheral and central retinal inflammation. Our patient had the retinal appearance of both PORN (central retinal lesions) and ARN (peripheral retinal involvement with intraocular inflammation), which are not infrequent.4 PORN is usually seen in immunocompromised patients.
Unfortunately our patient’s retinal condition was fulminant and antiviral medication therapy did not salvage vision.
Kyrieleis’ arteriolitis have been only rarely reported in patients with ARN.1 Kyrieleis’ plaques have been postulated to be due to calcific deposits in the arterial walls or migration of exudates from active choroiditis to the periarterial sheaths, with compartmentalisation of the exudates due to anatomical variations.1 ARN should be considered as a differential diagnosis when Kyrieleis’ plaques are observed.
If necrotising retinitis is suspected on clinical review aqueous sampling to include PCR of all herpesvirus (VZV, HSV (types 1 and 2), CMV and EBV) and syphilis serology are prudent. If the patient is unresponsive to antiviral therapy, consider alternative diagnosis such as lymphoma or toxoplasma. HIV testing is also suggested as opportunistic retinal infections can occur in HIV/AIDS. Aqueous humour sampling carries low risk in contrast to vitreous sampling. It is advised that vitreous should not be sampled unless as a part of formal three-port vitrectomy.5
Our patient was unaware that she was HIV positive. The very low CD4 count and high viral load suggest that the patient was infected with HIV >5 years previously and which chimed with her history of unprotected sexual encounters in Africa 5 years previously. It transpired that the patient had, at that time, attended the hospital because of genital herpes and was offered HIV testing at the time or after 2 months to cover the potential seroconversion window period. The patient opted to return to the genitourinary medicine clinic for testing after 2 months but did not attend for her follow-up appointment.
In our opinion, such unrecognised HIV infection predisposed her to the development of severe bilateral necrotising retinopathy from ophthalmic shingles. We are aware of one similar recent case report in the UK where PORN was described in the setting of unrecognised HIV.3 However, as that case did not present with shingles, we believe that our case may be unique in that regard. Furthermore, it may be timely to challenge the received wisdom that ARN is seen in the immune competent and that PORN is usually seen in patients who already have a diagnosis of HIV as the HIV may not have been diagnosed. It has become increasingly recognised that ARN and PORN are ends of a spectrum of necrotising herpetic retinopathy.
Neuroradiology of brain and orbits did not show any abnormalities in the visual pathway in our patient. High signals on MRI of optic nerves in such patients have been reported and has been postulated to be the reactivated virus migrating to the contralateral eye by axonal transport, through the optic nerves, to produce ARN syndrome in the fellow eye.6
The mainstay of treatment of necrotising herpetic retinopathy include long-term systemic antivirals, which include intravenous acyclovir 10 mg/kg three times a day for 7–10 days, then orally for 2–4 weeks. Oral valacyclovir 2000 mg four times daily was found to be comparable with intravenous acyclovir.7 Studies report benefits of combining systemic antivirals and intravitreal foscarnet therapy to reduce severe vision loss or reduce the incidence of RD.8 9 Flaxel et al reported that patients treated with combination therapy, intravenous acyclovir 10 mg/kg three times daily or oral valacyclovir 1000 mg three times daily with serial intravitreal foscarnet injections (2.4 mg/0.1 mL) every 3–4 days, until disease quiescence had reduced incidence of severe vision loss and RD.10 The American Academy of Ophthalmology (AAO) has recently published guidance on management of ARN.11 That review noted that while studies have shown that prophylactic laser retinopexy may have a role in preventing RD, however, due to selection bias, for example, eyes that received prophylactic laser in many cases had clearer media and better presenting VA and less involved retinitis than eyes that did not have laser, it is uncertain whether the prophylactic laser is of benefit.11 Early vitrectomy before RD has been postulated to remove inflammatory mediators, remove vitreous traction and allow the application of more complete laser demarcation to necrotic retina and the placement of long-acting tamponade to prevent subsequent RD. Based on the evidence of four studies that examined visual and anatomical outcomes after early vitrectomy before the RD development, the AAO review noted that it cannot be concluded whether vitrectomy to prevent RD in the setting of recent ARN is of benefit.11 Patients with rhegmatogenous RD secondary to viral retinitis who underwent pars plana vitrectomy with silicone oil and scleral buckle were found to have successful anatomical retinal reattachment with no recurrent RD, however postoperative vision was poor, possibly due to optic neuropathy.12 A recently published retrospective case series also reported disappointing visual outcomes in patients with ARN despite early pars plana vitrectomy surgery.13
Potential immunocompromised status should be considered in patients with shingles. Such patients should be questioned for activities that pose risk of blood borne viruses exposure. Such questions should include asking about sexual history, substance abuse, blood transfusion and travel history. ARN should be considered when Kyrieleis’ plaques are found on funduscopy. In patients with HZO reporting loss of vision do seek to detect retinitis, as aggressive antiviral treatment should be commenced to seek to reduce the risk of vision loss in the other eye. Importantly, if funduscopy is obscured in such shingles patients consider ruling out RD with ultrasound.
Learning points
Severe genital herpes or complicated herpes in any form warrants an HIV testing.
History of living in high-endemic areas for HIV even in a stable relationship warrants HIV testing by any healthcare professionals.
Potential immunocompromised status should be considered in patients with severe or recurrent shingles. HIV testing should be offered.
Progressive outer retinal necrosis may be a presenting sign of previously unrecognised HIV infection.
Viral retinitis should be treated aggressively to seek to preserve some vision and reduce risk to fellow eye.
Footnotes
Contributors BN and SPK: literature search, figures, data collection, data interpretation, writing up paper, proof reading, revision and final approval of version. CC: provided images, data interpretation, drafting of manuscript and final approval of version. EM: literature search, data collection, data interpretation, revision of paper and final approval of version.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.