Article Text

Statistics from Altmetric.com
Description
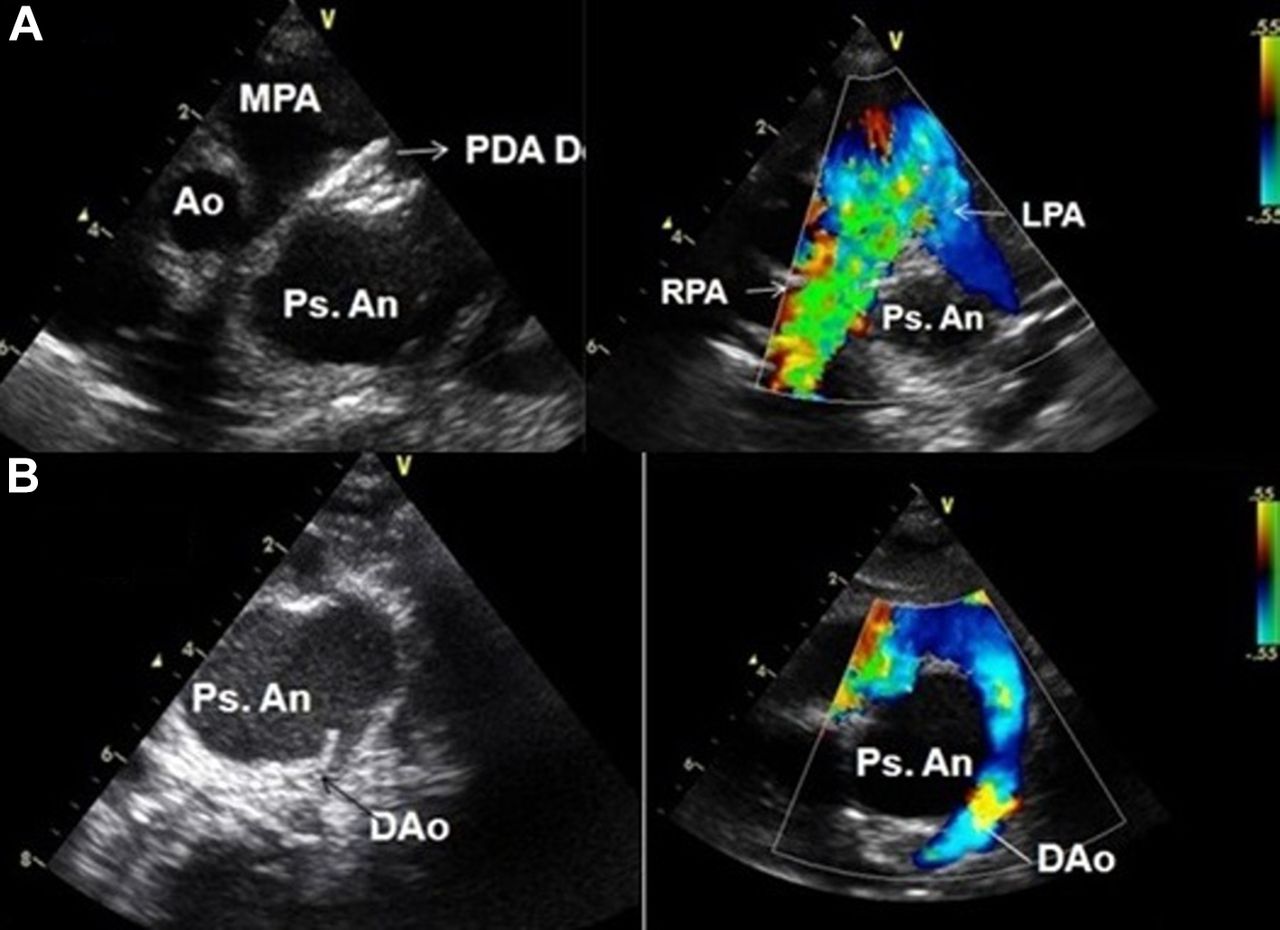
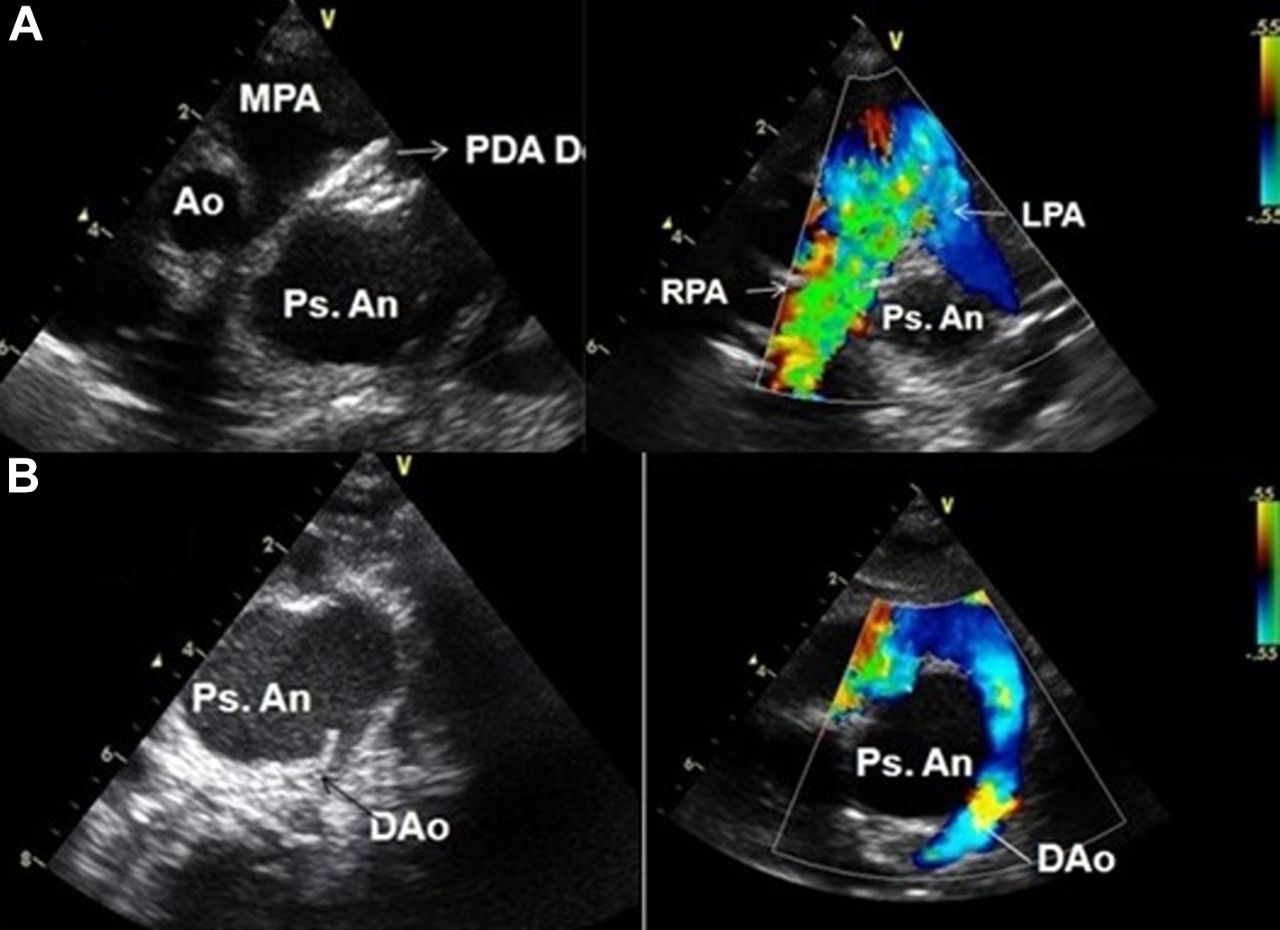
A 7-month-old girl, ex-preterm (26-weeker), 4.5 kg, with 4 mm patent ductus arteriosus (PDA) underwent PDA device closure (Amplatzer duct occluder - ADO II 4×6 mm) elsewhere and was readmitted 4 days later with pericardial effusion. Needle pericardiocentesis drained 50 mL of haemorrhagic fluid. Septic screen was negative. Severe dyspnoea ensued 2 weeks later. Chest X-ray excluded lung pathology. Bedside echocardiogram showed PDA device in situ (online supplementary video 1), no residual ductus, vegetation or pericardial recollection, unobstructed flow in the pulmonary artery and descending aorta, normal pulmonary arterial pressures, and normal biventricular function. Curiously, a giant anechoic mass (22×25 mm) (online supplementary video 2) was visualised posteroinferior to the device with its neck communicating with lesser curvature of the thoracic aorta at the level of origin of the left subclavian artery (figure 1A,B). Intra-aneurysmal thrombus or aortic dissection was absent. We diagnosed giant ductal pseudoaneurysm with possible left bronchial compression.
Supplementary file 1
Supplementary Material
{kind=link}
(A) Parasternal short-axis transthoracic two-dimensional echocardiogram showing patent ductus arteriosus (PDA) device (PDA D, indicated by arrow) with giant pseudoaneurysm (Ps. An) posteroinferior to it. Ao, aortic valve; MPA, main pulmonary artery. Right hand panel shows the colour Doppler image of preserved pulmonary arterial flows (LPA, left pulmonary artery; RPA, right pulmonary artery) without any residual ductus with the pseudoaneurysm (Ps. An) sandwiched between the two. (B) Modified suprasternal echo-colour Doppler showing the location of pseudoaneurysm (Ps. An) inferior to transverse arch and medial to the descending aorta (DAo) without any evidence of coarctation of aorta.
She underwent emergency surgical resection of pseudoaneurysm, retrieval of device, and reconstruction of pulmonary artery and aorta with homograft. Intraoperatively, perforation of proximal ductal wall by guidewire in the catheterisation laboratory was discovered. Fortunately, as the perforation leaked subacutely and the pseudoaneurysm was supported by the left pulmonary artery and left bronchus from above and below, respectively, it did not rupture.
This case highlights an uncommon sequel to a common paediatric intervention. New-onset haemorrhagic pericardial effusion is always a ‘red flag’, and serial, clinically focused echocardiography is required. To conclude, although PDA device closure has 93%–97% success rate,1 2 every intervention is still a challenge, and this is the first report of postdevice ductal pseudoaneurysm3 in infancy.
Patient’s perspective
When my preterm baby was diagnosed to have a hole in the heart called PDA, I was devastated. However, I was reassured that it may be closed even without surgery. But, when medicines did not close the PDA, I was advised regarding non-surgical closure with device. This did not turn out to be a great option as my child ultimately required a 6 hour massive surgery to correct the first procedure. I was told that this is a rarest of rare event but I hope it never happens to any baby again.
Learning points
A pseudoaneurysm/false aneurysm develops when the vascular wall is injured and the blood is contained by surrounding structures.
Trauma to patent ductus arteriosus (PDA) during PDA device closure must be avoided and the guidewires/device and others must be carefully manipulated.
New-onset haemorrhagic pericardial effusion occurring post cardiac intervention is always a red flag. Serial bedside echocardiography is enough to evaluate any unusual clinical presentation. We re-emphasise that there is no ‘routine intervention’ in paediatric catheterisation laboratory.
Footnotes
Contributors MC took care of the patient and wrote the manuscript. SVC contributed to management plan and writing. SSI was involved in discussions and writing. DS was the operating surgeon.
Competing interests None declared.
Patient consent Guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.