Article Text

Statistics from Altmetric.com
Description
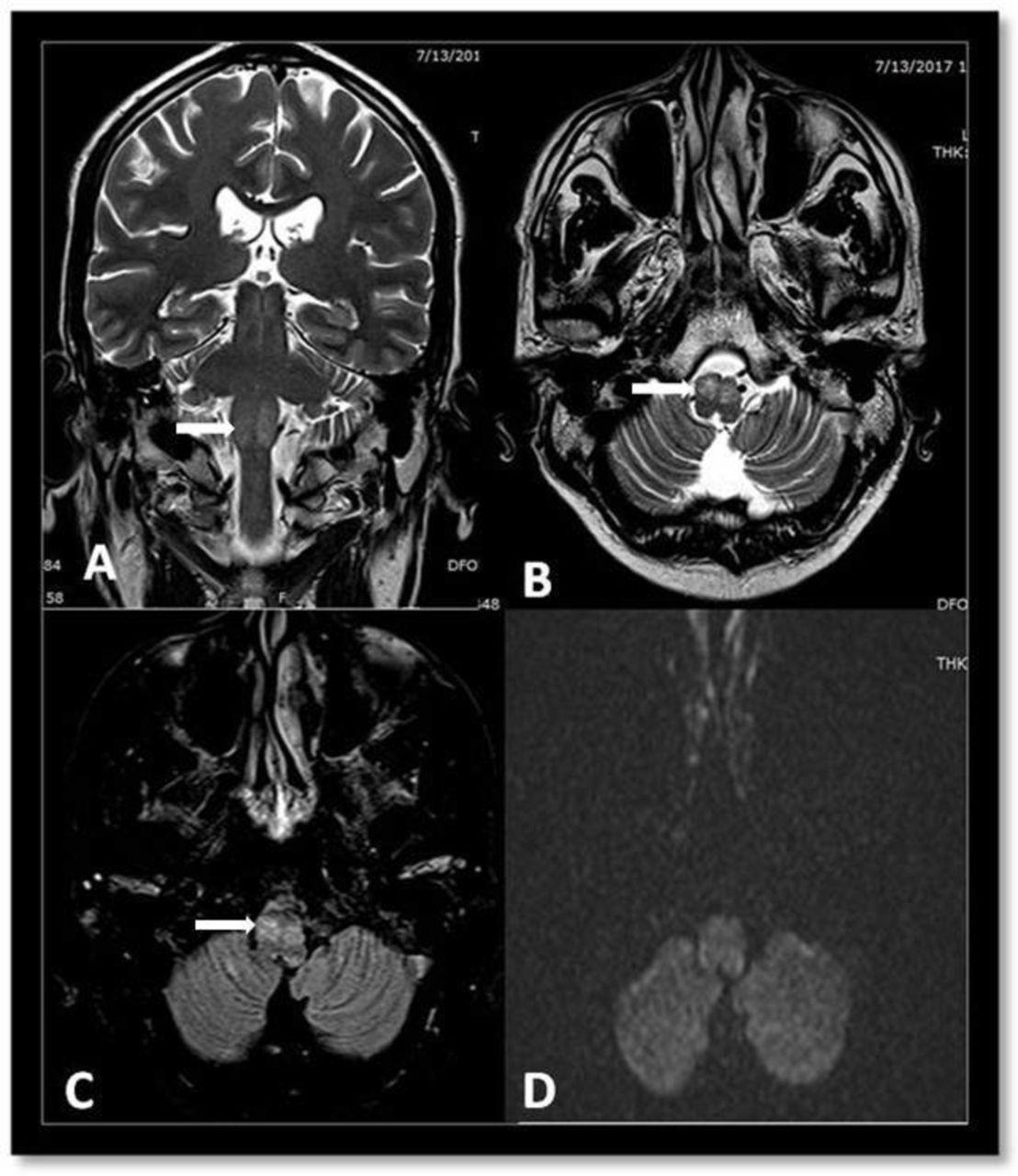
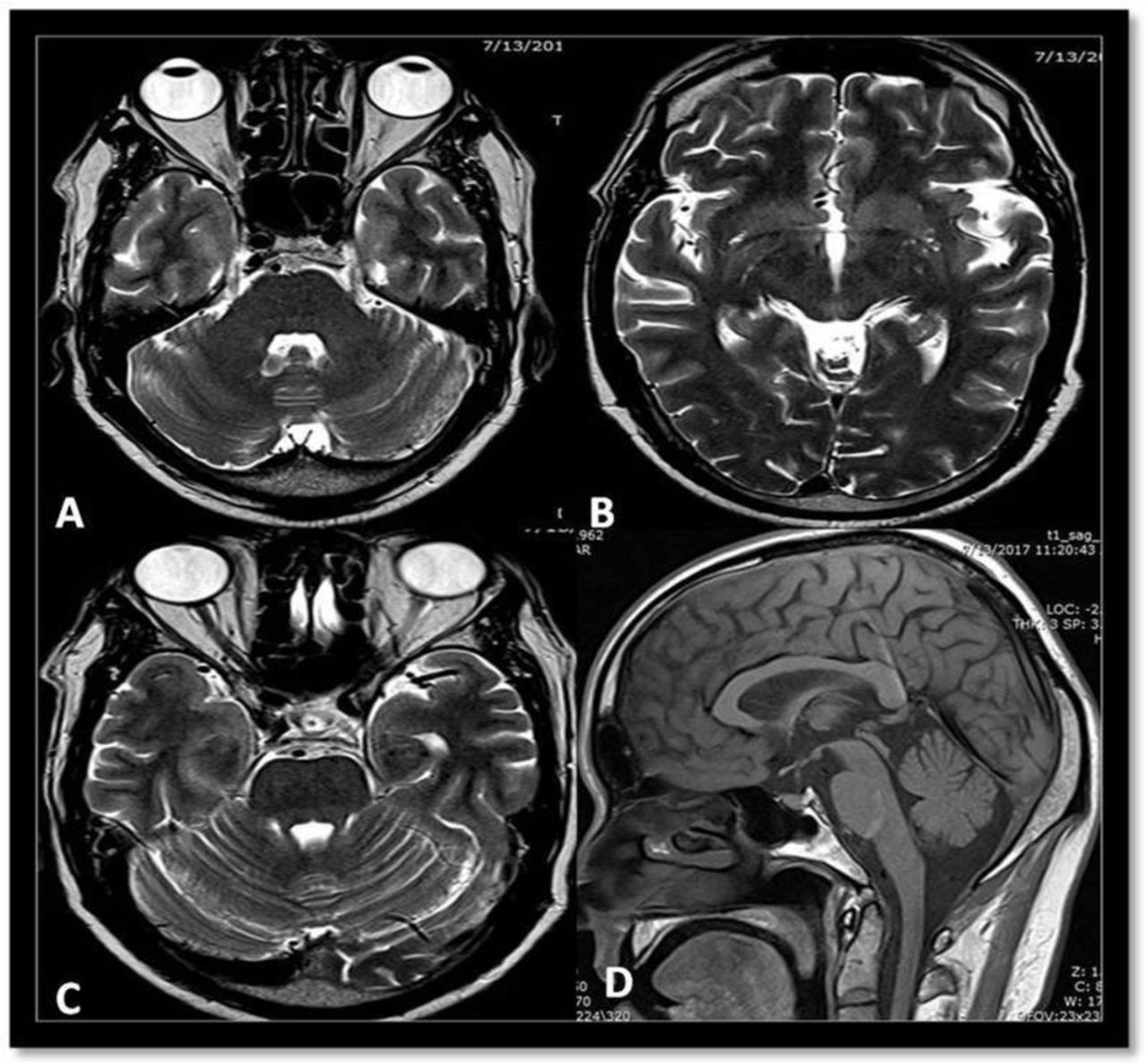
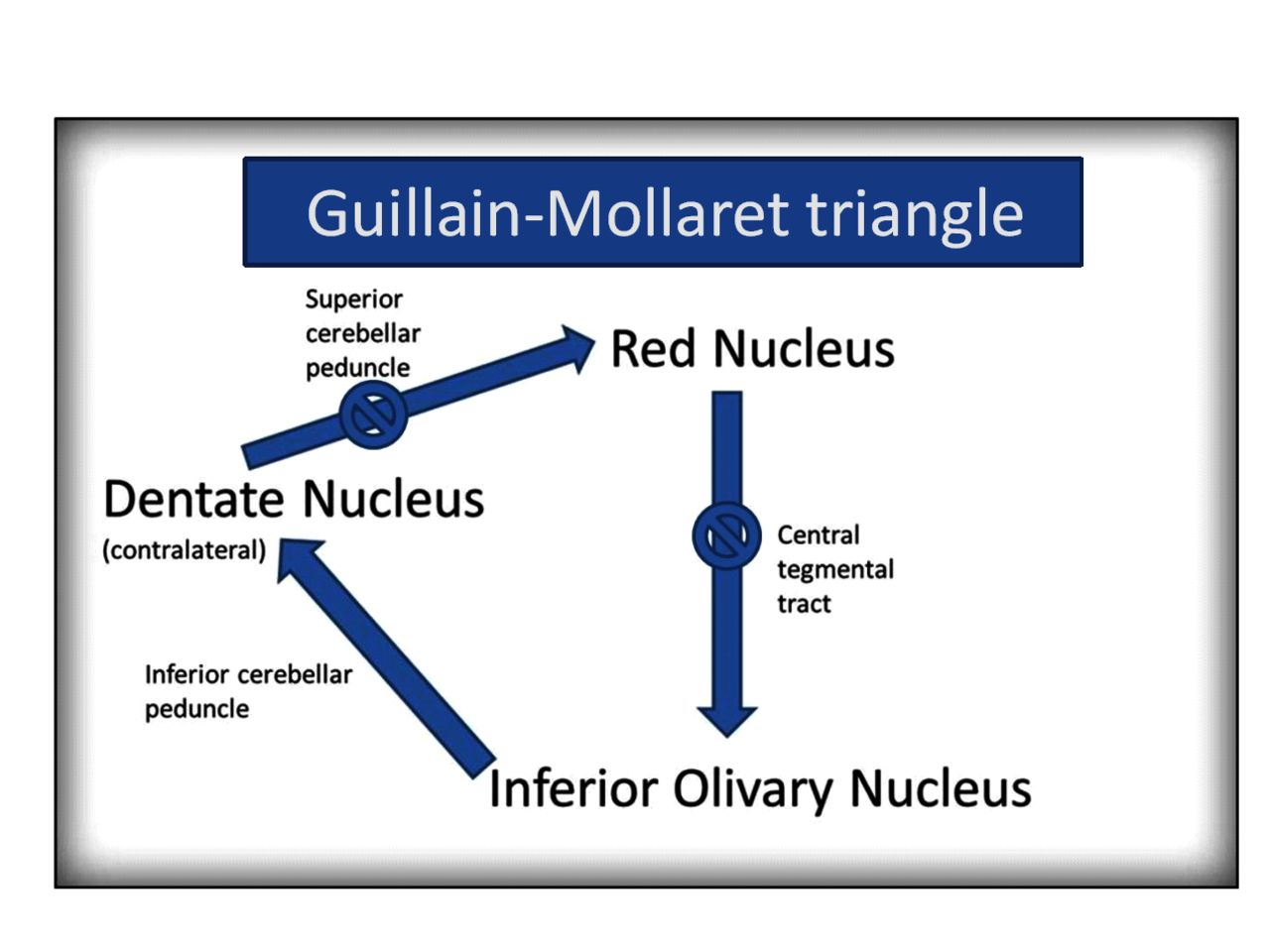
A 55-year-old man presented with involuntary movements of the tongue and soft palate associated with unsteadiness in walking for a period of 3 months. The patient did not complain of ear clicking. Examination revealed palatal myoclonus, tongue fasciculation and ataxic gait. MRI of the brain showed increased T2 and Fluid Attenuation Inversion recovery (FLAIR) signal intensities in the bilateral inferior olivary complex without diffusion restriction (figure 1). Midbrain, pons, and cerebral and cerebellar parenchyma were normal (figure 2). Imaging features were consistent with bilateral hypertrophic olivary degeneration. Hypertrophic olivary degeneration is a unique type of trans-synaptic neuronal degeneration caused by damage to the dentatorubral pathway or the triangle of Guillain and Mollaret (figure 3). Focal lesions like infarction, haemorrhage, demyelination and trauma involving this neuronal pathway lead to interruption, and following sequential pathological changes are described (table 1).1

Coronal T2 (A), axial T2 (B), axial Fluid Attenuation Inversion Recovery (FLAIR) (C) and axial diffusion (D) showing enlarged hyperintense inferior olivary nucleus (white arrows) with no diffusion restriction.

Axial T2 (A,B,C) and sagittal T1 (D) MRI of the brain showing normal midbrain, pons, and cerebral and cerebellar hemispheres.

{kind=link}
{kind=link}
{kind=link}
Illustration of Guillain and Mollaret triangle. Disruption (crossed circle) of dentatorubral tract or central tegmental tract can result in trans-synaptic degeneration of the inferior olivary nucleus.
Sequential pathological changes in hypertrophic olivary degeneration
Hypertrophic olivary degeneration is mostly bilateral, and half of bilateral cases may be implicated to primary neurodegenerative process.2 Our patient’s MRI revealed no abnormality involving the Guillain and Mollaret triangle. Hence the exact cause for hypertrophic olivary degeneration is not known. According to a study conducted by Gu et al, one in every five patients of hypertrophic olivary degeneration was idiopathic, and most of the idiopathic cases were showing bilateral hypertrophic olivary degeneration.3
Learning points
Hypertrophic olivary degeneration is a rare and unique type of neuronal degeneration mostly due to infarction, infection, demyelination and postsurgery and trauma.
Bilateral hypertrophic olivary degeneration is more common than unilateral involvement.
Majority of idiopathic (non-lesional) hypertrophic olivary degeneration is bilateral.
Footnotes
Contributors MV: conception and design, acquisition of data or analysis and interpretation of data. SVC: drafting the article or revising it critically for important intellectual content. PPN: final approval of the version published. UBS: agreement to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.