Article Text

Statistics from Altmetric.com
Description
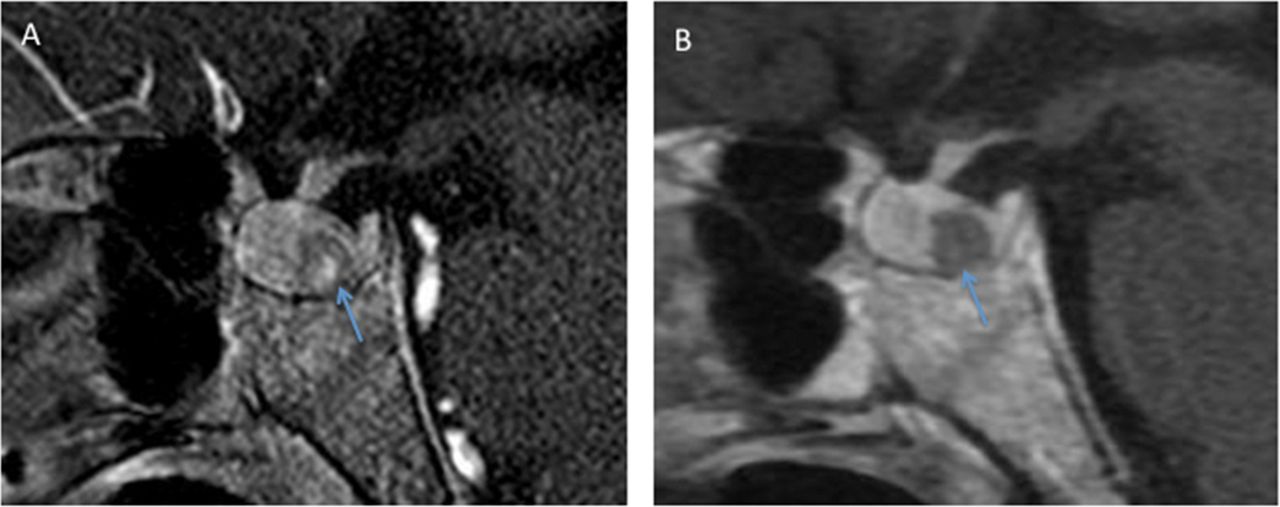
A 29-year-old woman with neurofibromatosis 1 (NF1) due to NF1 gene deletion presented for evaluation of long-standing secondary amenorrhea. She noted increasing growth of her hands and feet, inability to fit her ring on her fingers and increasing shoe size (currently US size 12). Physical examination revealed coarse and asymmetrical facial features, arthropathy with large hands and feet and multiple café-au-lait lesions. Biochemical evaluation was consistent with growth hormone (GH) and prolactin excess. Pituitary MRI with T1-weighted images showed a voluminous and symmetrically enlarged gland (overall dimensions 15×9×13 mm), with a heterogeneous hypointense lesion within the posterior pituitary, measuring 6×6×10 mm (figure 1A, arrow). On the fluid-attenuated inversion recovery and T2-weighted images, the lesion was markedly hypointense (not shown). There was no radiographic evidence of optic pathway tumours. Due to both elevations in GH and prolactin, it was decided to treat her acromegaly with cabergoline. A follow-up pituitary MRI was obtained 2 months after initiation of therapy that showed reduction in pituitary size and enlargement of the hypointense lesion (figure 1B). The abnormality within the pituitary is most consistent with a Rathke’s cleft cyst, a benign, epithelium-lined intrasellar cyst that is a remnant of the Rathke pouch (arrows). The cyst slightly increased in size following the reduction in pituitary volume from cabergoline therapy. GH excess in patients with NF1 is extremely rare but may be under-recognised.1 Indeed, acromegaly most often arises from a single GH-secreting pituitary adenoma; however, in certain genetic syndromes that predispose to the development of various tumours, such as NF1 or Carney’s complex, generalised mammosomatotroph hyperplasia can be seen, as in this case.2 After 2 months of cabergoline therapy, the patient noted a reduction in her ring size.
{kind=link}
(A) Pituitary MRI with T1-weighted images with contrast showing a voluminous and symmetrically enlarged gland (overall dimensions 15×9×13 mm), with a hypointense lesion within the posterior pituitary, measuring 6×6×10 mm (figure 1A, arrow). (B) Follow-up pituitary MRI with T1-weighted images with contrast on a different machine was obtained 2 months after initiation of cabergoline therapy showing a reduction in pituitary size (overall dimensions 12×8×10 mm) and enlargement of the hypointense lesion measuring 9×9×12 mm.
Learning points
A Rathke’s cleft cyst is a benign epithelium-lined intrasellar cyst that is a remnant of the Rathke pouch.
Growth hormone (GH) excess in patients with NF1 is extremely rare and arises from a single GH-secreting pituitary adenoma or generalisedmammosomatotroph hyperplasia.
Footnotes
Contributors All authors participated in the work as a whole and reviewed and agreed with the content of the article.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.