Article Text

Statistics from Altmetric.com
Description
A 69-year-old man with known, stable atypical meningioma of the brain diagnosed 5 years previously presented with severe shortness of breath. The patient had previously been treated with surgery and radiotherapy to the brain. Chest X-ray revealed bulky mediastinal lymphadenopathy (figure 1). CT (figure 2) confirmed mediastinal and upper abdominal lymphadenopathy in addition to multiple pulmonary emboli. The patient underwent an endoscopic ultrasound and fine-needle aspiration (EUS-FNA), an established technique that enables prompt cytological sampling and assessment.1

Chest X-ray.

Contrast-enhanced CT image showing adenopathy at the level of the aortic arch.
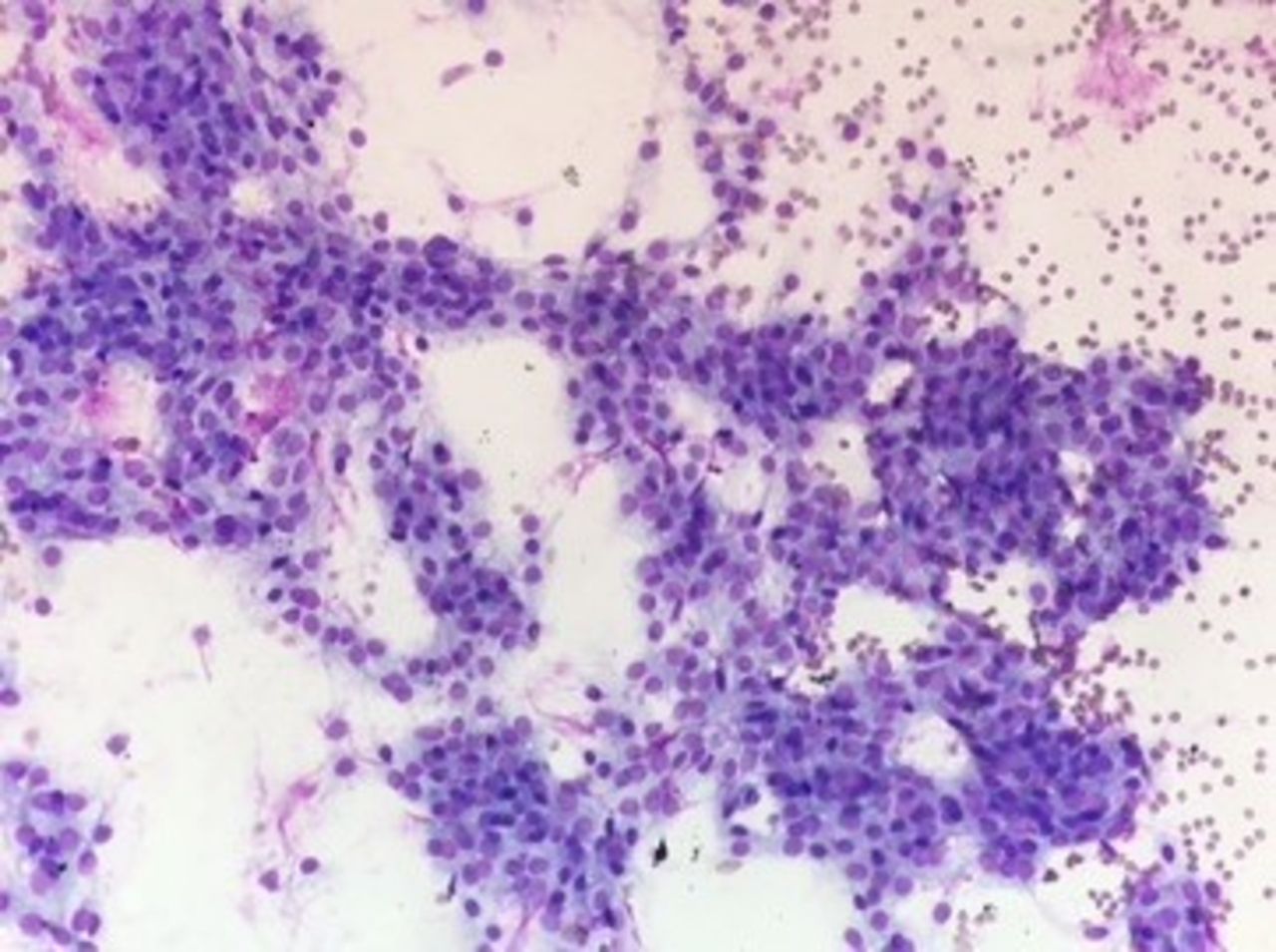
The EUS-FNA preparations showed sheets and clusters of bland, polygonal epithelioid cells (figure 3). These demonstrated strong immunohistochemical positivity (figure 4) for epithelial membrane antigen. The final immunopanel was strongly supportive of metastatic meningioma.

Endoscopic ultrasound and fine-needle aspiration cytology preparation with Giemsa stain showing bland sheets and clusters of polygonal meningioma cells.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical stain showing diffuse tumour cell positivity for epithelial membrane antigen.
Meningiomas are common intracranial tumours, classified by WHO into three grades based on mitotic activity and tumour differentiation.2 Atypical (grade 2) and anaplastic (grade 3) meningiomas account for less than 5% of all meningiomas, and metastases from these lesions are rare (0.1%).3
Due to the small number of patients with a diagnosis of metastastic meningioma, there are no established treatment pathways and the prognosis is unknown.3
The patient in our case report completed radiotherapy to the mediastinum at a dose of 30 Gy in 10 fractions over 10 days, which improved his respiratory symptoms alongside a reducing dose of steroids. Following clinic discussion, he declined systemic treatment options and opted for palliative care.
To the best of our knowledge, this is the first case in the literature of metastatic meningioma diagnosed through EUS-FNA.
Learning points
Extracranial metastases from atypical meningioma are rare.
Evidence-based treatment options are limited.
Endoscopic ultrasound and fine-needle aspiration can enable prompt cytological diagnosis of enlarged lymph nodes and lesions from a variety of locations in the thorax and abdomen.
Acknowledgments
The authors would like to acknowledge the following peoplefor their contribution to the case study: Dr Dushyant Shetty (ConsultantRadiologist) for reviewing the radiologyimages, Ms Leonie Glinski (Senior Biomedical Scientist in Cytology) forproviding the cytology images, and Dr Aditya Shivane (Consultant Neuropathologist)for guidance regarding the patient’s original diagnosis and metastaticpresentation.
Footnotes
Contributors HLB and EMOH contributed equally to this paper. JEG is the consultant histopathologist who reported the cytology and reached the correct diagnosis. FGM is the consultant clinical oncologist who managed the care of the patient. Both JEG and FGM provided critical appraisal of the final article.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.