Article Text

Statistics from Altmetric.com
Description
A 53-year-old woman presented to the emergency department (ED) with a 3-day history of gradual onset left-sided headache localised behind the left eye. This was associated with visual disturbance in the left eye described as ‘zig-zag lines’.
She had never suffered from headache before and her only significant medical history was of hysterectomy and subsequent provoked pulmonary embolus. She was not taking any regular medication.
Initial assessment was completed by an Foundation Year 2 doctor (FY2) in ED. There was no evidence of focal neurological deficit. A diagnosis of migraine with aura was reached and the patient was discharged home with a short course of non-steroidal anti-inflammatories and paracetamol. She was advised to return to the ED if her symptoms failed to improve or in the event of new symptoms developing.
She returned the following day. The patient was again assessed by an FY2 in ED. The description of her headache had not changed. However, on this occasion, she had developed ptosis, meiosis and on further examination anhydrosis (Horner’s syndrome). Her case was discussed with a senior ED clinician who advised urgent neuroimaging was required.
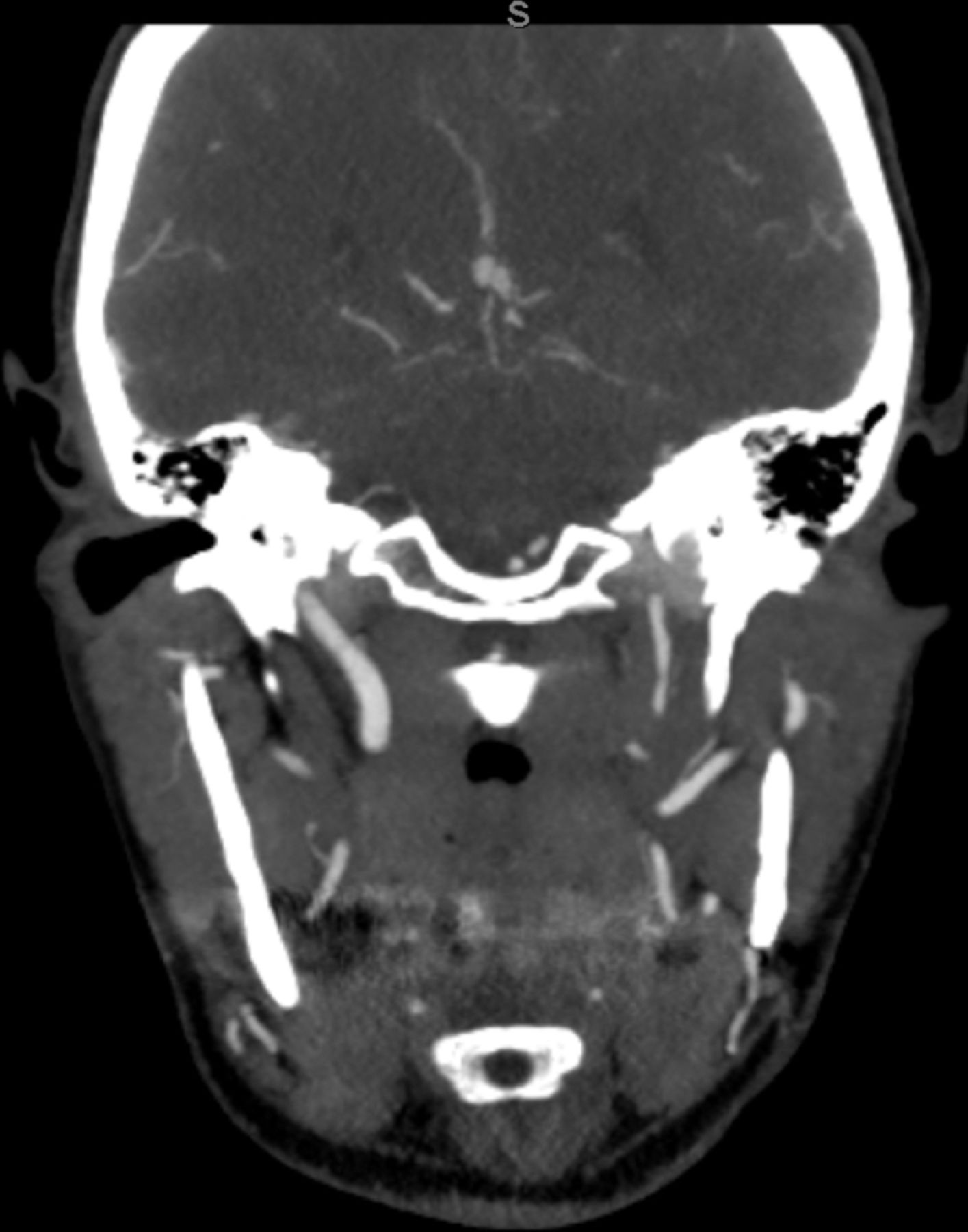
Non-contrast CT brain was normal. However, CT angiography revealed an extensive left internal carotid artery (ICA) dissection (figure 1) with associated pseudoaneurysm (figure 2).
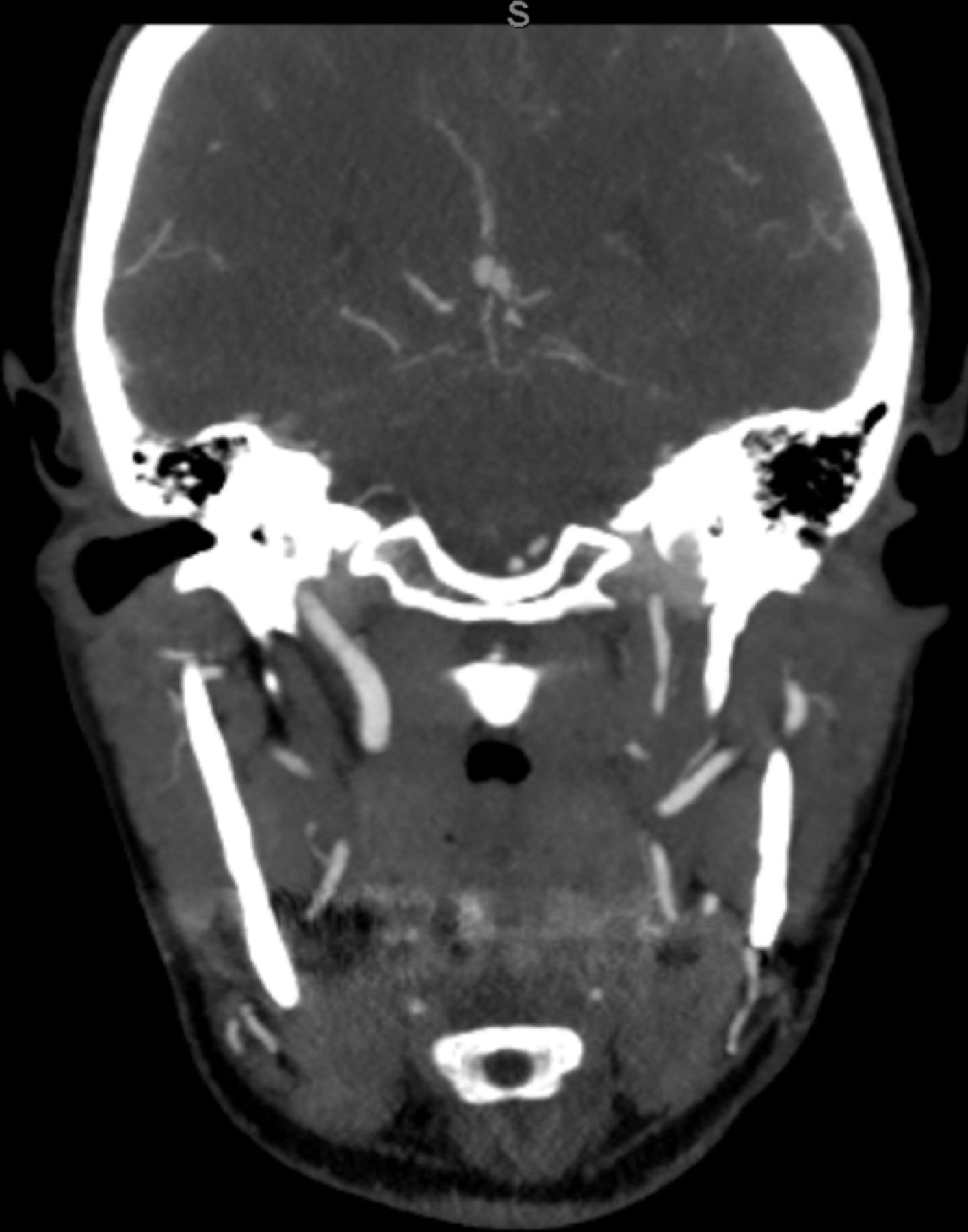
Coronal view of CT angiography showing significant luminal narrowing of the left ICA from the level of C2 throughout the left carotid canal with a string-like and tortuous appearance, likely due to dissection.

{kind=link}
{kind=link}
Reconstructed CT angiography showing the pre-petrous segment of the ICA with luminal narrowing and a small pseudoaneurysm measuring 4 mm x 6 mm.
The finding of left ICA dissection necessitates urgent anticoagulation due to the strong association between arterial dissection and thromboembolic disease including stroke.1 2
Other stroke risk factors were assessed including blood pressure, lipid profile and fasting glucose. She started on both lipid-lowering and blood pressure medication as a result. The patient was also advised about modifiable lifestyle factors such as diet and exercise.
Her headache continued to be managed by using simple analgaesia.
Ongoing follow-up was arranged at the Stroke Outpatient Clinic. At the time of last review, the patient was asymptomatic. Further follow-up imaging is awaited at time of writing this case report.
In retrospect, it is clear that the patient’s first presentation at the ED did not meet criteria for migraine with aura. As per the International Classification of headache Disorders, the following diagnostic requirements were not met:
Two separate attacks were not reported.
Full reversibility of aura symptoms had not been demonstrated.
Somewhat confusingly, however, “Headache or facial or neck pain attributed to cervical arterial dissection is usually unilateral (ipsilateral to the dissected artery), severe and persistent (for a mean of 4 days). However, it has no constant specific pattern and it can sometimes be very misleading, mimicking other headaches such as 1. Migraine, 3.1 Cluster headache or 4.4 Primary thunderclap headache”.3
Learning points
It is important to seek specialist input from a neurologist in cases of headache that do not meet diagnostic criteria for primary headache.
‘Safety-netting’ advice in the emergency department is of importance.
There is an urgent need for anticoagulation in patients diagnosed with carotid artery dissection.
Footnotes
Contributors The patient was seen in the emergency department upon representation by AD. When final diagnosis was made, the case was discussed by BS and AD and a decision to write the case up was made. BMJ Case Reports journal was identified as an appropriate publication. The case was written up based on the BMJ Case Reports model by AD and proof-read by BS. AD is acting as corresponding author. RB was heavily involved in helping to address comments raised during the peer review process. IR is the reporting radiologist.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.