Article Text

Statistics from Altmetric.com
Description
A 44-year-old African-American woman presented to the emergency department with chest pain and shortness of breath of 12 hours prior to presentation. Her medical history includes antithrombin deficiency, recurrent deep venous thrombosis (DVT), recurrent pulmonary emboli, poorly controlled hypertension, diabetes mellitus, asthma, inferior vena cava filter placement, pulmonary hypertension and bipolar disorder. Her surgical history includes bilateral pulmonary thromboendarterectomy 3 months prior to presentation. She reported non-compliance to Coumadin. She smokes half a pack per day for the last 25 years. Family history is positive for multiple early deaths secondary to thromboembolic complications.
Physical examination showed tachycardia with heart rate of 105 beats per minute. Chest examination was significant for bilateral rales at the lung bases. ECG showed sinus tachycardia, cardiac troponins were negative and international normalised ratio was 1.08. Venous duplex of the lower extremities showed chronic DVT.
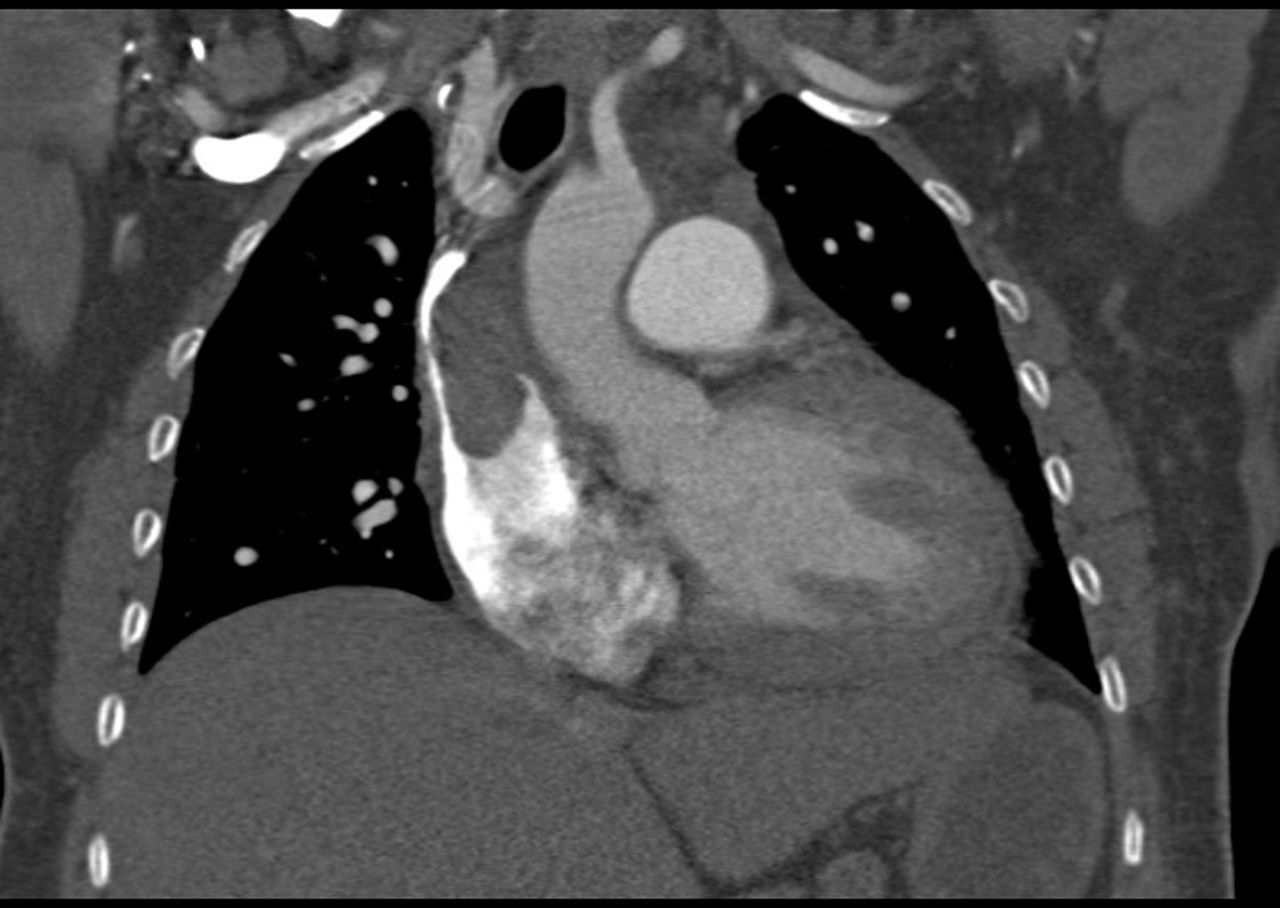
Chest CT scan with contrast showed an occlusion of the left brachiocephalic vein surrounding a Mediport catheter with a large thrombus extending into the superior vena cava and right atrium (figure 1). The superior vena cava was not completely occluded. CT also showed right lower lobe segmental pulmonary arterial thromboembolism. Patient was advised to stay on lifelong enoxaparin injections 1.5 mg/kg and was referred to a tertiary cardiac surgery centre for surgical intervention. She underwent clot removal. She was maintained on enoxaparin with no further thromboembolic complications for 2 years follow-up.
{kind=link}
CT of the chest with contrast showing occlusion of the left brachiocephalic vein surrounding the Mediport catheter with large thrombus seen within the superior vena cava hanging into the superior vena cava and part of the right atrium. The thrombus is measuring 4.7×2.1 cm in size.
Antithrombin is a potent inhibitor of thrombin and other coagulation serine proteases.1 Antithrombin deficiency is a hereditary thrombophilia which is inherited as autosomal dominant with variable penetrance.1 Antithrombin deficiency lifetime probability of developing thrombosis was 8.1 times higher than those without the defect.2 Long-term anticoagulation is indicated for high-risk patients with recurrent thromboembolic episodes.3
Learning points
Patients with antithrombin deficiency are at higher risk of thromboembolic episodes.
Identifying patients with antithrombin deficiency is crucial for prevention and treatment of thromboembolic complications.
Footnotes
Contributors KW, AA and ZA edited the case and reviewed the related literature. SAH wrote the case, reviewed the related literature and accepted the final version.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.