Article Text

Summary
Renal infarction is a rare occurrence accounting for 0.007% of patients seen in the emergency department for renal insufficiency or hypertension. Dysfibrinogenemia is also rare, and the combination of renal artery infarct in the setting of congenital dysfibrinogenemia has not been described in the literature. Our patient, with a remote history of congenital dysfibrinogenemia with no known haemorrhagic or thrombotic complications, presented with acute flank pain and was subsequently diagnosed with an acute renal arterial infarction. He was treated with subcutaneous enoxaparin and then transitioned to lifelong anticoagulation with rivaroxaban therapy.
- haematology (incl blood transfusion)
- renal medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Renal infarction is a rare occurrence. In a study performed by Paris et al, patients evaluated for renal insufficiency or hypertension were found to have acute renal infarction in 0.007% of cases.1 The incidence of infarction is likely underestimated due to underascertainment, as renal colic is often treated as nephrolithiasis or pyelonephritis without advanced imaging studies. Rarer still is acute renal artery infarction in the setting of congenital dysfibrinogenemia. Congenital dysfibrinogenemia is a disorder, which can result in acute haemorrhages or infarctions as a result of a thrombus. It is the result of an autosomal-dominant inherited point mutation resulting in a dysfunctional protein. Although the majority of mutations are silent, haemorrhagic and thrombotic events do occur (25% and 20%, respectively).2 Because of the rarity of the condition, not many cases are reported specifically with an acute renal infarction. We present a case that highlights the importance of medical thoroughness in both patient history and disease pathophysiology.
Case presentation
The patient is a 37-year-old Caucasian man, with a medical history of exertional rhabdomyolysis, dysfibrinogenemia (diagnosed several years after increased bleeding from a dental procedure), morbid obesity, obstructive sleep apnoea (OSA) and postural orthostatic tachycardia syndrome, presented to our institution after having 4 days of acute left back pain that has progressively worsened with radiation to the left flank. He had presented 2 days prior where, in the emergency room, he was found to be afebrile, haemodynamically stable without lab abnormalities and a normal non-contrast CT scan of his abdomen and pelvis (figure 1). He stated that his pain began after exercising, initially characterised as a dull ache that was minimally alleviated with ibuprofen and a heating pad. On his current presentation, the pain was characterised as a sharp stabbing flank pain with intermittent cramping that was not alleviated by non-steroidal anti-inflammatory drugs or positional change. In the emergency department, he was found to be afebrile, hypertensive and in acute distress secondary to the debilitating flank/lower back pain he was experiencing.

Non-contrast-enhanced CT of the abdomen and pelvis. This study was acquired the day prior to acute presentation when the patient was admitted for infarction. The right kidney is normal without evidence of hydronephrosis or nephrolithiasis. The left kidney is normal without evidence of hydronephrosis or nephrolithiasis. No ureterolithiasis is identified.
Investigations
Laboratory evaluation was significant for normal creatine kinase, creatinine, lipase and liver-associated enzymes. Urinalysis was within normal limits. Coagulation studies revealed an elevated prothrombin time (18.3 s), elevated thrombin time (26.2 s), a high normal partial thromboplastin time (34.9 s) and a low fibrinogen (100 mg/dL). Given the acute change in pain, his history of dysfibrinogenemia and concerning coagulation panel, a contrast-enhanced CT scan of his abdomen and pelvis was performed. The contrast-enhanced CT scan revealed a posterior-lateral left upper renal pole infarction with non-opacification of an associated posterior segmental artery, bilateral main renal arteries and veins were evident (figure 2). These findings are consistent with acute clotting leading to ischaemia, as opposed to haemorrhage-based infarction.

Contrast-enhanced CT of the abdomen and pelvis. One day following initial presentation, a contrast-enhanced CT scan was performed in the nephrographic phase. Coronal reconstruction through the kidneys demonstrates a wedge-shaped perfusion deficit in the upper lateral left kidney.
Differential diagnosis
The patient’s initial presentation of flank pain has a broad differential diagnosis. Early in the case, nephrolithiasis was the leading diagnosis given the exquisite flank pain that did not resolve with position changes. However, urinalysis did not reveal microscopic haematuria, and recent non-contrast CT was negative for calculi or hydronephrosis. Given the patient’s medical history of rhabdomyolysis and recent intense exercise, acute rhabdomyolysis was also considered but excluded based on a normal creatine kinase level. With no acute urinary complaints of hesitancy, frequency or dysuria and no objective evidence of infection (no fever, no leucocytosis, benign urinalysis and no fluid collections on radiography), acute urinary tract infection or occult abscess was low on the differential diagnosis. Prior to the contrast CT, musculoskeletal exacerbation of a previous injury, such as an insult to the psoas or quadratus lumborum muscles, was also considered.
On follow-up imaging, radiology suggested a possible aneurysm, which expanded the differential diagnosis to also include infarction due to dissection in addition to the diagnosis of renal artery infarction due to thrombus formation or embolism. Spontaneous renal artery dissection and/or aneurysm is quite rare, with an incidence of <0.05% with approximately only 180 cases having been reported.3 In a longitudinal study of 438 patients with renal infarction, 21 patients had renal artery dissection or aneurysm, and 29 patients had hypercoagulable states.4 Given the rarity of the spontaneous dissection and aneurysm and the high prevalence of thrombus formation in natural history of congenital dysfibrinogenemia and no evidence of dissection on initial contrast-enhanced study, renal artery infarct due to thrombus formation or embolism was more likely. Furthermore, further review of the imaging demonstrated a vessel at the level of incident with the same diameter before and after the severe stenosis, less indicative of aneurysm or dissection.
Treatment
The patient was admitted for anticoagulation, pain control and consultation for possible acute vascular intervention. He was started on a heparin infusion, pain medication and intravenous hydration. Interventional radiology and vascular surgery services determined that no intervention was required given no laboratory evidence of kidney damage, and the patient continued to make sufficient urine. Dalteparin was initially considered by haematology department, though there were concerns for dosing in the setting of morbid obesity, and enoxaparin was selected. An echocardiogram was performed showing no atrial thrombus, an ejection fraction of 60%–65% and mild pulmonary hypertension. The hospital course was uncomplicated. By the fourth hospital day, he was transitioned to oral pain control and deemed medically ready for discharge, with planned outpatient follow-up with haematology department to discuss duration of anticoagulation.
Outcome and follow-up
At his follow-up visit, he was no longer experiencing back or flank pain, and a contrast CT scan was done to evaluate for infarct resolution (figure 3). Follow-up imaging initially raised suspicion of a segmental pole renal artery aneurysm (figure 4). However, further evaluation of the imaging determined that an aneurysm was not present (figures 5, 6). The patient also had a genetic work-up for congenital dysfibrinogenemia and was found to be heterozygous for FGA gene (fibrinogen alpha), as genetic analysis was not part of his initial work-up. Given the patient’s young age, no history of bleeding despite having dysfibrinogenemia and a large unprovoked infarction, it was determined that the risk–benefit ratio favoured indefinite anticoagulation using rivaroxaban with follow-up every 6 months.

Contrast-enhanced CT of the abdomen and pelvis. Ten weeks following initial presentation, a contrast-enhanced CT angiography was performed to evaluate the renal arteries. Coronal reconstruction through the kidneys during the arterial phase demonstrates evolution of the renal infarct as evidenced by interval renal parenchymal volume loss and persistence of the perfusion deficit without evidence of aneurysm.

Contrast-enhanced CT of the abdomen and pelvis. Ten weeks following the initial contrasted study, a repeat was performed for reassessment. On the initial read, a small renal artery aneurysm arising from a segmental renal artery within the upper pole of the left kidney coming off the main renal artery was identified. This finding was later contested.

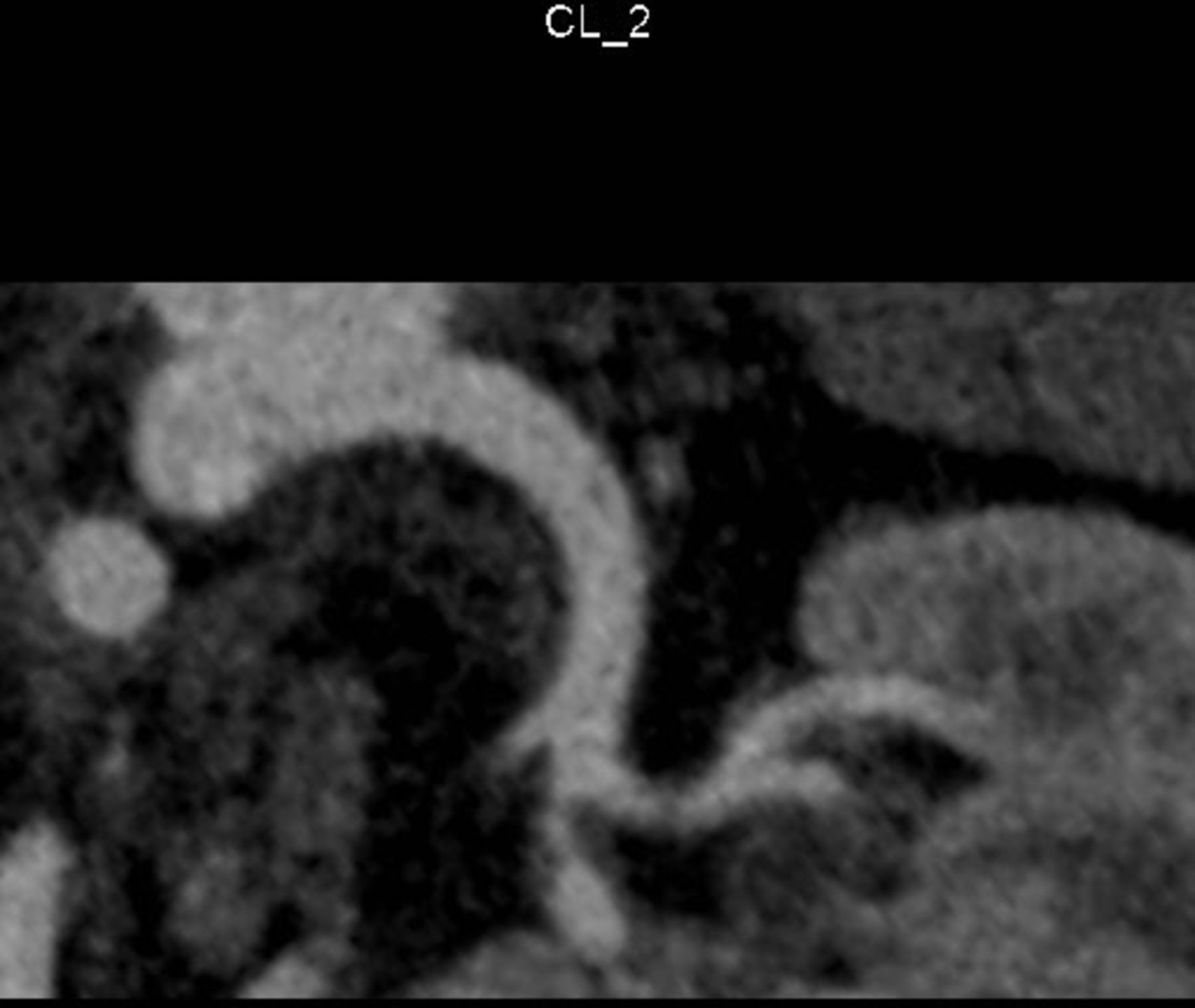
CT angiogram of the left renal artery. Ten weeks following initial presentation, a contrast-enhanced CT angiography was performed to evaluate the renal arteries. Curved multiplanar reformation was constructed using a computer-generated centre line through the main and involved segmental renal artery. Focal concentric non-calcified plaque is seen in the proximal portion of a segmental branch of the main renal artery where it causes qualitatively severe stenosis. Findings were confirmed on the transaxial images. There is no evidence of aneurysm.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT angiogram of the left renal artery. Ten weeks following initial presentation, a contrast-enhanced CT angiography was performed to evaluate the renal arteries. Curved multiplanar reformation was constructed using a computer-generated centre line through the main and involved segmental renal artery. Quantitatively the stenosis was measured as 85% maximal percent diameter stenosis, without evidence of precipitating aneurysm.
Discussion
Generally, renal infarction is the result of either cardiovascular dysfunction, such as atrial fibrillation, or a predisposition to thromboembolic events. In one analysis, cardiogenic caused 55.7% of cases, renal injury accounted for 7.5%, hypercoagulable state contributed 6.6% and idiopathic was the cause for remaining 30.1%.4 Congenital dysfibrinogenemia is a rare disease state that can be inherited in an autosomal-dominant, codominant or even autosomal-recessive pattern affecting the FGA, fibrinogen beta or fibrinogen gamma genes that can result in thrombotic or haemorrhagic events. There have been more than 100 mutations identified, over 90% of which are point missense mutations, that result in the phenotype of abnormal fibrinogen. Prevalence of congenital dysfibrinogenemia is unknown as many cases are subclinical. The large number of mutations, limited statistics about risk and lack of specific clinical practice guidelines makes treatment decisions challenging and individualised.
Dysfibrinogenemia can also be acquired. The most common cause of acquired dysfibrinogenemia is liver disease, where the synthetic function of the liver results in dysfunctional fibrinogen leading to bleeding and thrombotic complications.5 Patients may also develop antibodies to fibrinogen which has been reported in patients with systemic lupus erythematosus, ulcerative colitis, multiple myeloma and therapy with isoniazid.6 These antibodies can block fibrinopeptide release, fibrin monomer polymerisation or fibrin crosslinking.6 Antibody-associated acquired dysfibrinogenemia cases lend themselves to haemorrhage as opposed to thrombosis.6 In diagnosing acquired dysfibrinogenemia, patients often have no history of bleeding or clotting, and family history is not significant for haematological events. The patient will have a temporal relation to an underlying diagnosis of acquired rather than congenital. In liver-associated acquired dysfibrinogenemia, fibrinogen levels are usually normal, as opposed to congenital dysfibrinogenemia, where fibrinogen levels are low normal to deficient. In addition, genetic testing of patients with acquired dysfibrinogenemia will not reveal any mutations associated with the congenital variant.
Currently, venous thromboembolisms secondary to congenital dysfibrinogenemia should be treated with low-molecular-weight heparin.7 Long-term treatment recommendations have not been established due to the rarity of the condition and the lack of data to support superiority of any one treatment modality.7 When considering long-term therapy, being either to initiate or not to initiate any specific treatment or choosing between anticoagulants, it is imperative to take into consideration all the variables of the patient. In our particular case, the patient was young and presented with clinically significant infarction, we felt as did the patient, that the benefit of instituting lifelong anticoagulation significantly outweighed the risks of non-treatment or short-term treatment.7 Of the treatments currently available, Coumadin was anecdotally successful for long-term treatment.8 However, in discussion with the patient, rivaroxaban was, instead of Coumadin, initiated to increase medical compliance, considering the increased drug surveillance and the disruption that would incur on his life.
Dysfibrinogenemia can manifest as a bleeding disorder or thrombotic disorder. The variant that a patient suffers from is based on the mutation they have and other genetic variables that are beyond the scope of this case report. In a review by Casini et al, the cumulative incidence rate of major bleeding was determined to be 19.2%, and cumulative incidence rate for thrombotic events was determined to be 30.1%. In a review of 250 reported cases, 26% had bleeding, and 21% of cases had venous or arterial thrombosis.7 Of the 48 patients that suffered from bleeding events secondary to dysfibrinogenemia followed by Casini et al, 29.4% had menorrhagia making it the most common, 20.8% of patients had cutaneous bleeding, and 8.9% had bleeding after surgery. Four patients suffered from gastrointestinal bleeding and one developed spontaneous haemarthrosis. In the Casini et al study, 28 patients developed thrombosis, with 20 venous events and 8 arterial events. Venous events were varied, having 11 deep venous thromboses, 3 pulmonaryembolisms, 2 superficial vein thrombophlebitis events and 4 thromboses at unusual sites reported. The arterial events included four strokes, two acute myocardial infarctions, one peripheral artery occlusion and one mesenteric artery thrombosis. Casini et al concluded reported incidence of venous thromboembolisms of 5.58/1000 patient-years, which is greater than that reported in the general population (1.5/1000 patient-years).7 Given this high incidence, high clinical suspicion needs to be given for haemorrhage or thrombus when evaluating patients with dysfibrinogenemia with non-specific symptomatology in an acute setting.
In this particular case, the question of aneurysm as possible aetiology for the infarction was raised after follow-up contrast CT scan of the abdomen and pelvis revealed a possible small aneurysm in the upper pole of the left renal artery (figure 3). However, this finding was reviewed further and was determined that an aneurysm was not present. This is evidenced in figures 5 and 6 with no dilation of the vessel, no dissection of the vessel wall and no saccular deformity to the vessel. Through this arterial phase imaging and curved multiplanar reformation reconstruction of the kidney, we can say with a high degree of certainty that aneurysm is not present and therefore could not have led to the renal infarction.
Despite the potential hazards of dysfibrinogenemia, a majority of cases are clinically asymptomatic and are discovered incidentally via routine blood work. In a study by Haverkate and Samama, 138 of 250 (55%) patients with congenital dysfibrinogenemia were diagnosed after routine coagulation studies prompted further investigations.9 In the Casini et al study of 101 patients, the majority (39/67, 58%) had an incidental diagnosis.7 Currently, there is not enough information to determine a mortality benefit of prompt genetic testing and diagnosis in symptomatic or asymptomatic congenital dysfibrinogenemia, given the rarity of the condition and the lack of evidence to support treatment and prophylaxis guidelines.
Renal artery infarction is a late diagnosis in the general population because most do not have a predisposition to thrombosis through either congenital or cardiac causes. When evaluating a patient with congenital dysfibrinogenemia, a low threshold for diagnosis needs to be used as it has the potential to decrease morbidity and mortality through earlier diagnosis. If the infarction is not treated promptly or treated at all, patient can develop renal injury or depending on the extent of infarction, loss of the kidney. Systemically, patients can develop hypertension, uraemia, acidosis and electrolyte imbalance, in the acute phase.
Learning points
Dysfibrinogenemia is a rare disorder characterised by primarily missense mutations, leading to a non-functional protein structure.
A large proportion of patients with dysfibrinogenemia manifest with haemorrhagic complications, but can also present with thrombosis or infarction.
Flank pain has a broad differential, but with careful history and physical examination, proper diagnosis, even rare aetiologies such as renal artery infarction, will not be missed.
Lifelong anticoagulation in these patients is a case-by-case basis. More evidence is needed to define definitive treatment.
Acknowledgments
Although not listed, we would like to recognise Dr Brian Fogarty who was integral to the evaluation of the images crucial to solidifying the aetiology of the case.
Footnotes
Contributors All authors served as editors of the article. JP and BS served as mentors and advisers. KK and TC took direct care of the patient presented in the case report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.