Article Text

Summary
Pseudocoarctation is an unusual anomaly mirroring true coarctation. Congenital kinking or pseudocoarctation of aorta was never a benign condition. Although surgical repair should be suggested for all symptomatic individuals. Regular follow-up is obligatory for all asymptomatic patients deprived of linked anomalies. We suggest CT-aortogram as a non-invasive imaging modality for the definitive diagnosis of pseudocoarctation.
- cardiovascular medicine
- medical education
- radiology (diagnostics)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Pseudocoarctation of the aortic arch is an infrequent congenital anomaly which can be inferred as an anomalous elongation of the aorta in superior mediastinum and may be misguided for true coarctation of aorta or superior mediastinal malignancy. It is characterised by kinking or buckling of the descending aorta at the level of the ligamentum arteriosum lacking a pressure gradient across the lesion.1 2 This case was diagnosed with second-degree uterovaginal prolapse, cystocele and rectocele. The patient was referred to us for routine cardiac evaluation which uneventfully turned out to be a pseudocoarctation. We report here an unusual presentation of pseudocoarctation of the aorta.
Case presentation
A 39-year-old woman presented with second-degree uterovaginal prolapse, cystocele and rectocele to the department of gynaecology in our institution. She was referred to us for preanaesthetic cardiac evaluation.
Physical examination revealed symmetrical blood pressure of 130/80 mm Hg in both arms and a pulse delay of 160 ms at radio-femoral arteries. So there was a suspicion of coarctation of aorta which warranted further investigations.
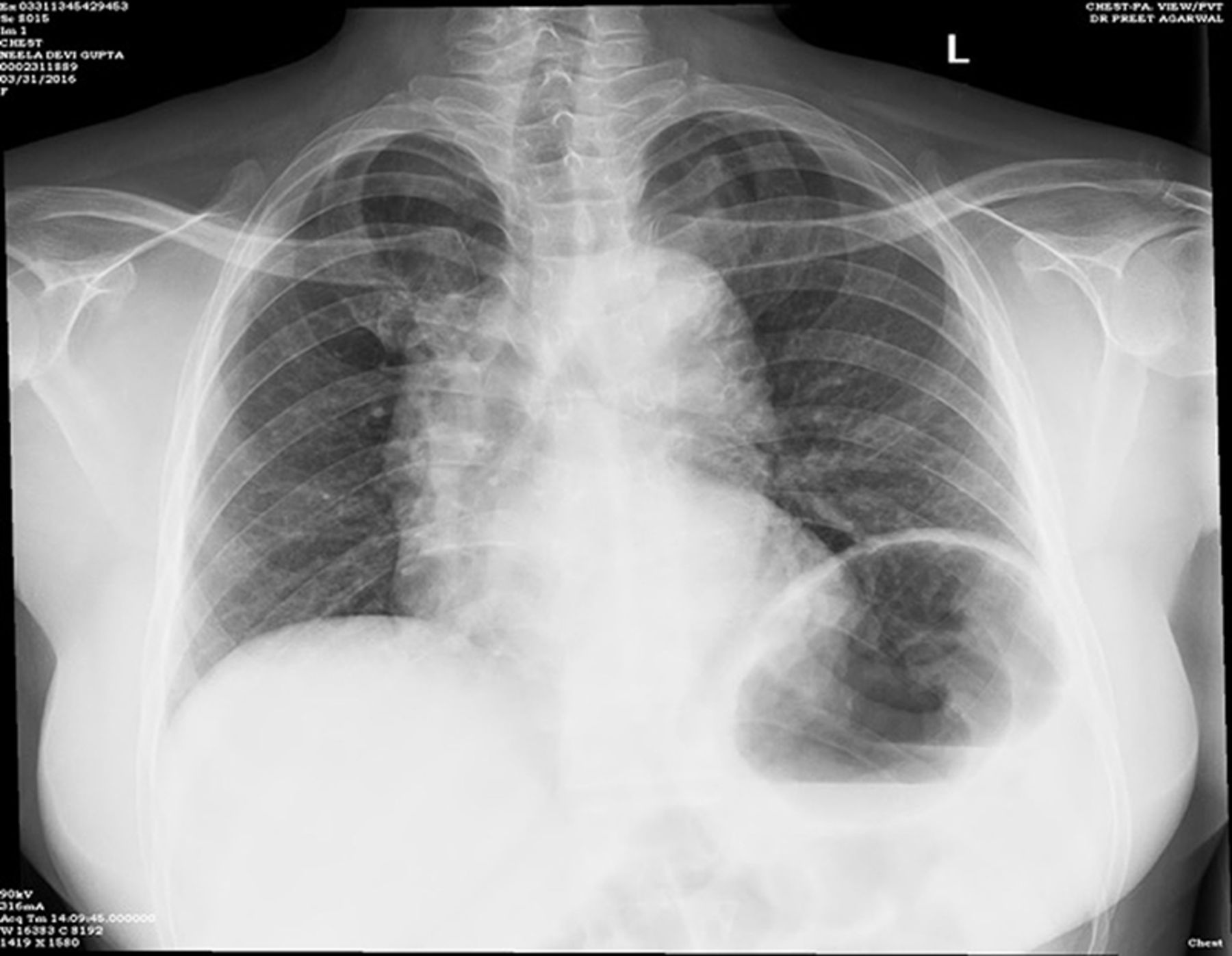
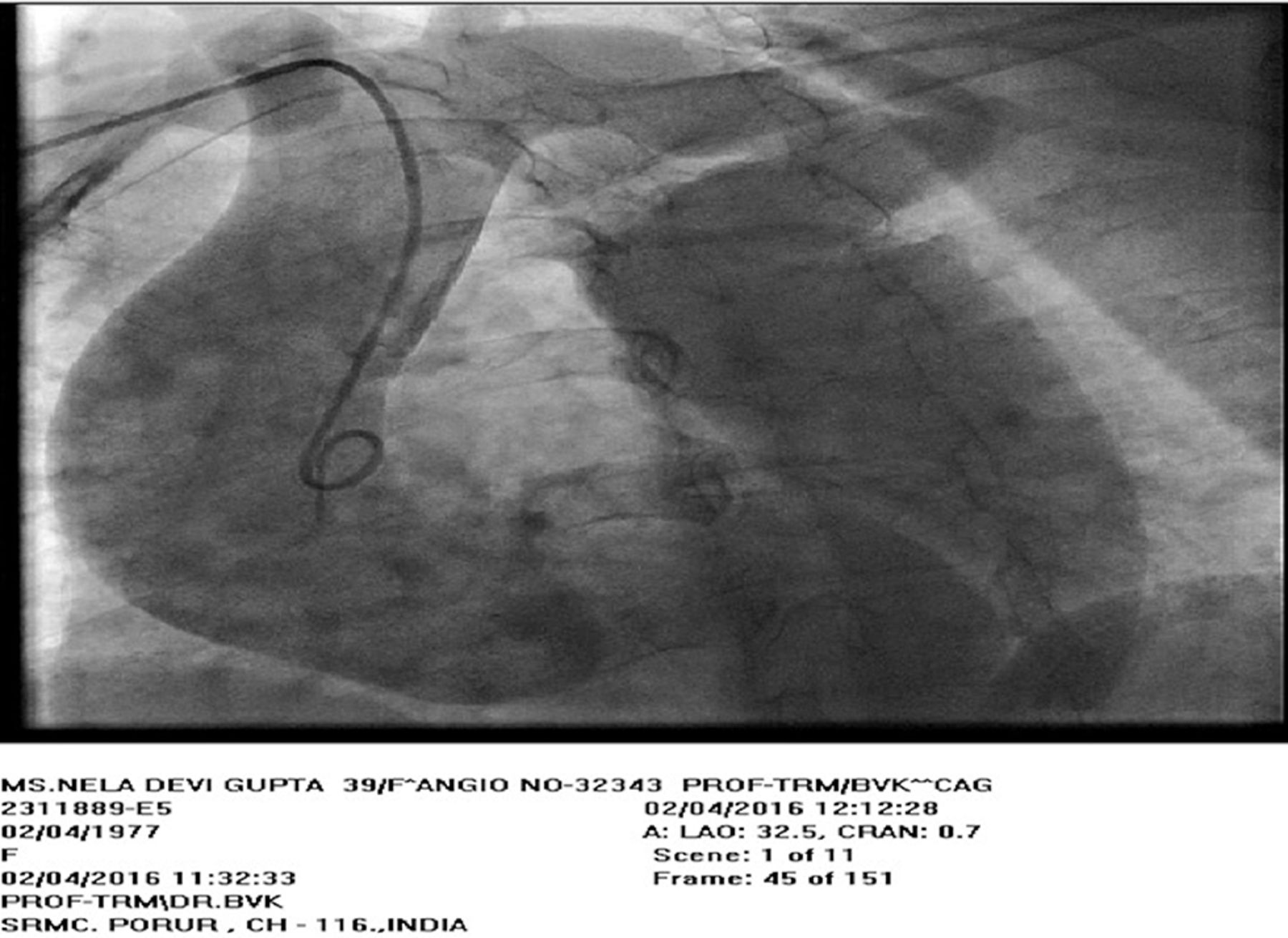
Echocardiogram showed normal left ventricle ejection fraction and normal aortic valve structure without any pressure gradients. X-ray chest disclosed a twofold shadow in the aortic arch representing number ‘3’ sign (figure 1). CT aortogram of the thorax further defined a lengthened aortic arch, luminal tapering distal to the left subclavian artery, poststenotic dilation and pseudo-3 pattern with measurements of aortic root—27.2 mm; ascending aorta—34.8 mm; kinking segment—14.3 mm; descending aorta—37.6 mm (figure 2). No rib notching or collateral circulation was noted, coherent with aortic pseudocoarctation. Coronary angiogram revealed the division past left common carotid up to left subclavian artery is lengthened and tortuous with kinking, and no pressure gradients was noted across the kinking segment (figure 3).

Chest X-ray (posteroanterior view).
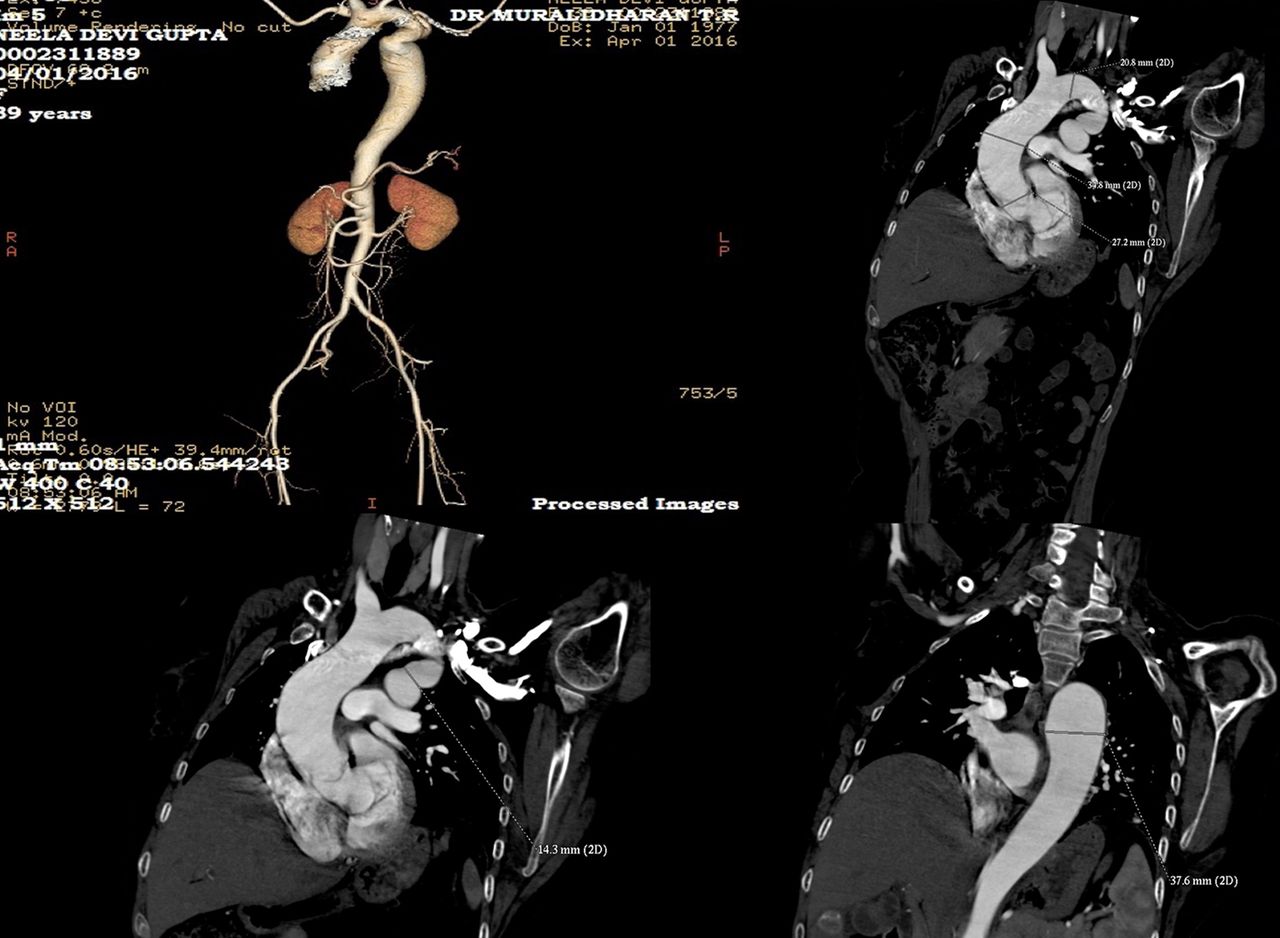
CT-aortogram (three-dimensional image) with measurements.

{kind=link}
{kind=link}
{kind=link}
Aortic angiogram.
Investigations
CT-aortogram.
Discussion
Pseudocoarctation of aorta is an unusual congenital elongation and kinking of the aorta, without significant pressure gradient between extremities or increased collateral circulation, differentiating it from true coarctation. Its precise aetiology is not well acknowledged. A theory stated as embryological origin in a failure of compression of the third through the seventh segments of the dorsal aortic roots and the fourth arch segment.3 Gay and Young proposed the diagnostic criteria4 and included a peculiar chest X-ray (left superior mediastinal shadow, in our case consistent to the pseudo-3 sign), lack of pressure variance between the upper and lower extremities (<25 mm Hg), no proof of increased collateral circulation (eg, rib notching).
No other congenital anomalies such as patent ductus arteriosus, ventricular septal defect, bicuspid aortic valve, aneurysm of the Valsalva sinuses and corrected transposition.
Pseudocoarctation is mostly asymptomatic and, as in our case, can be predictable on X-ray chest posteroanterior view.5 Recognising this variant is crucial as management is conservative.6 In our patient, good clinical skills, with meticulous interpretation of investigations, finalised the diagnosis of congenital kinking of aorta, and she was discharged after pelvic floor repair with appropriate medical treatment and she is in regular follow-up.
Patient’s perspective
I was diagnosed with a rare heart condition, which was completely explained to me with the nature, incidence, course, complication and treatment of this disease.
I had been asked to regularly follow-up in Department of Cardiology (Sri Ramachandra Medical Institute, Chennai).
The approach and management of all the doctors during the course of treatment was completely satisfactory.
Learning points
A thorough clinical examination and high clinical suspicion is needed in diagnosis of pseudocoarctation.
Patients with pseudocoarctation can have asymptomatic presentation.
Clinical management of symptomatic patients or asymptomatic patients with complication needs a definitive surgical repair.
Footnotes
Contributors MTR and SAND contributed to the conception or design of the work. VKB evaluated acquisition, analysis of case report. HSK did the drafting the work or revising it critically for important intellectual content.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.