Article Text

Statistics from Altmetric.com
Description
A patient in their 30s presented with a 3-day history of lower back pain, lower limb weakness and new onset of urinary incontinence. The patient had a history of metastatic melanoma, including to brain, for which they had previously been treated with adjuvant chemotherapy and radiotherapy. Clinical exam revealed a palpable bladder at the umbilicus and reduced power in the lower limbs bilaterally.
An MRI whole spine with gadolinium contrast agent revealed multiple enhancing lesions at the T5/6, T9 and T12–L3 levels, pronounced spinal cord oedema and a markedly distended bladder (figures 1 and 2). The location of these lesions within the spinal canal was mixed, including intramedullary metastases (ie, within the substance of the spinal cord) and intradural extramedullary metastases (ie, in the subarachnoid space but extrinsic to the cord). Lesions obliterated the cauda equina resulting in a cauda equina syndrome.

T2 sagittal MRI of cervical and thoracic spine. The white arrows demonstrate the typical appearance of intradural intramedullary spinal metastases with intense surrounding vasogenic oedema noted in the adjacent spinal cord (yellow arrow).
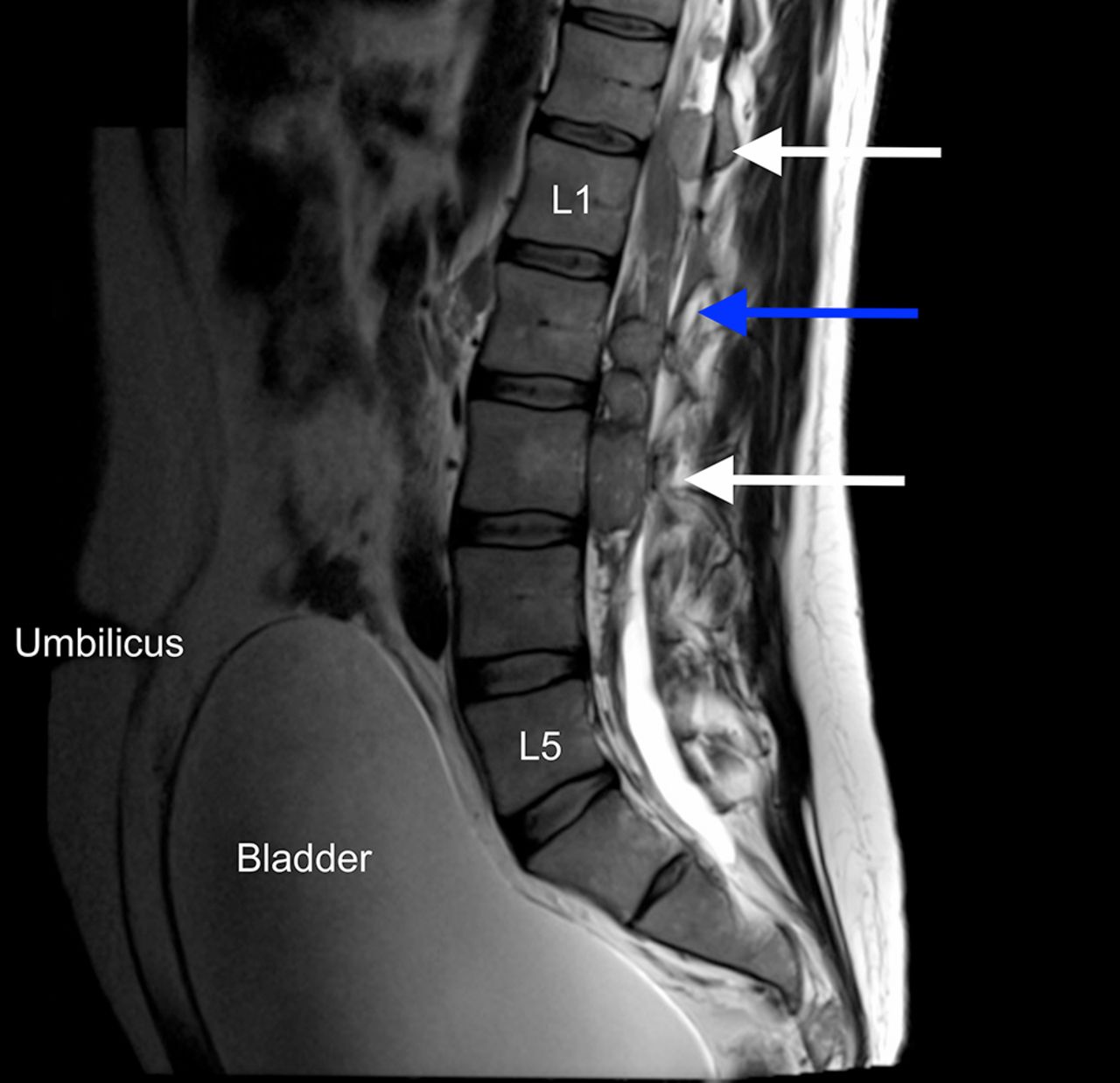
T2 sagittal MRI of the lumbar spine. The white arrows show multiple intradural extramedullary metastases in the region of the cauda equina (blue arrow). The bladder is massively distended to the level of the umbilicus, in keeping with the patient’s presenting complaint of urinary incontinence (overflow).
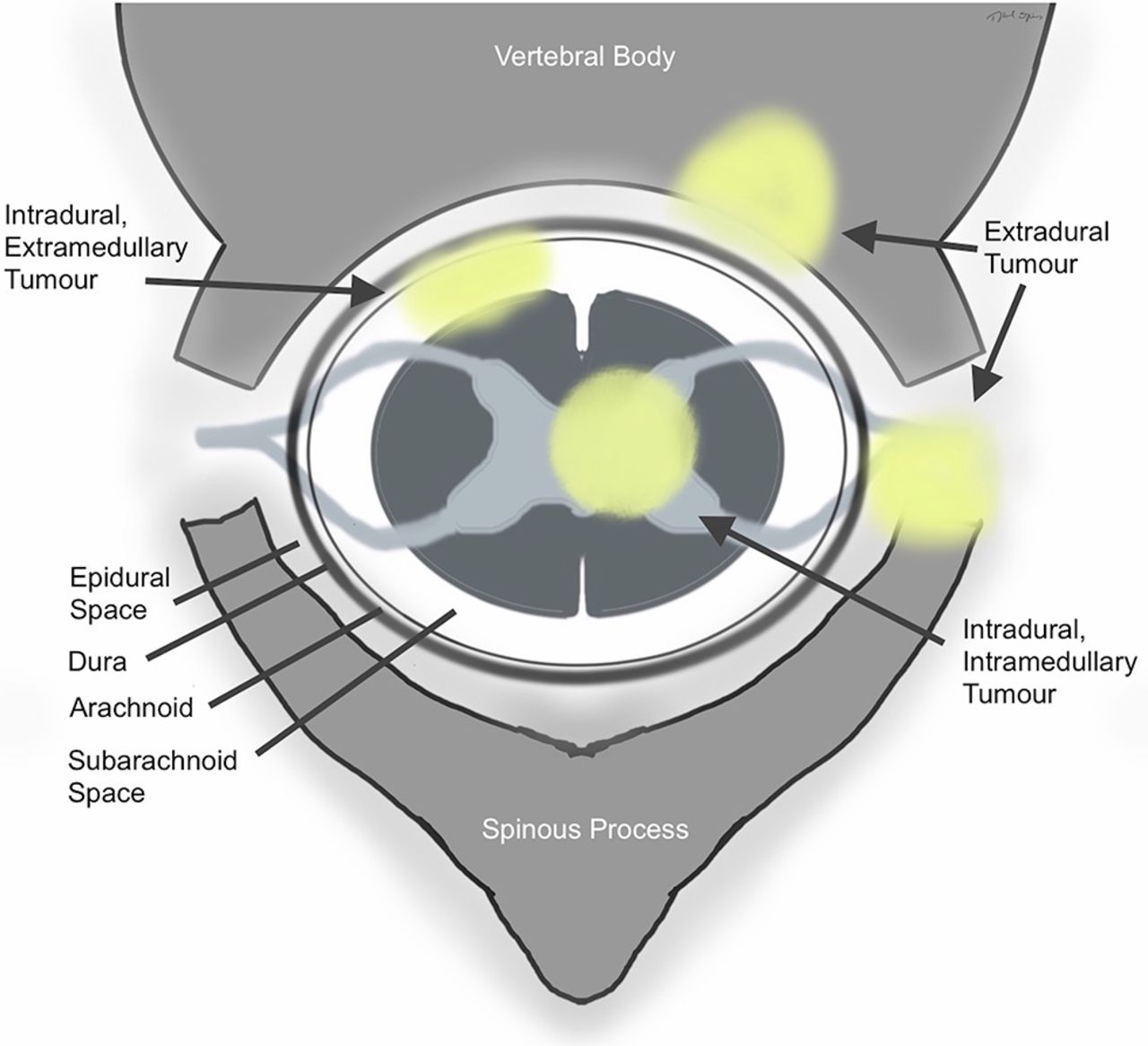
The three possible locations for spinal metastases are intradural intramedullary, commonly shortened to intramedullary, intradural extramedullary and extradural (figure 3). To our knowledge, this is the first reported case of mixed intramedullary and intradural extramedullary spinal cord metastases from malignant melanoma.

{kind=link}
{kind=link}
{kind=link}
The possible anatomical locations for spinal metastases.
Spinal extradural metastases affect up to 10% of all patients with cancer.1 Intradural metastases are rare but as systemic therapy improves their incidence has been reported to be on the increase.2 Lung, brain and breast cancer metastases are among the most common.2
Intradural spinal cord metastases have four proposed routes of spread that include (1) haematogenous—arterial and through the venous plexus (of Batson), (2) in the cerebrospinal fluid—‘drop metastases’, (3) in the central canal, involving the perineural lymphatics or (4) invasion from adjacent structures.3
The patient received immediate high-dose steroids, external beam radiotherapy and was started on pembrolizumab, a humanised monoclonal immunoglobulin. On follow-up at 3 months, the patient had regained bladder control and power in his legs, but died 10 months later from complications of the disease.
Learning points/take home message
Spinal cord metastases are not a single entity. They have three distinct possible anatomical locations: intramedullary, intradural extramedullary and extradural.
Extradural spinal cord metastases are the most common location. Concomitant intradural and extradural metastases are uncommon.
In the evaluation of neurological symptoms in patients with malignant melanoma, it is important to assess for intracranial metastases and intradural spinal lesions.
Footnotes
Competing interests None declared.
Patient consent Not obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement MOR was involved in the conception, data acquisition, writing and design of the manuscript. GS, DB and PM were involved in the conception, writing and editing of the manuscript. All authors have reviewed the final version and approved it.